

Translate this page into:
Plasmapheresis in Hypertriglyceride-induced Pancreatitis: A Series of Four Cases
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Hypertriglyceride-induced Acute Pancreatitis is a devasting condition. The rapid reduction of serum triglyceride is a key factor in its management. Beside the reduction in Triglyceride level plasmapheresis has other added advantage. Early initiation of plasmapheresis within 48 hrs has a better outcome. Plasmapheresis should be performed until triglyceride levels have been lowered to 500mg/dl. Here, we present a series of four cases of hypertriglyceride induced pancreatitis who underwent plasmapheresis. All the patients were diabetics. All cases showed the rapid reduction of triglyceride levels after plasmapheresis. Three patients were discharge from hospital, where as one patient died due to Sepsis. Out of four patients only one required Renal Replacement therapy
Keywords
Hypertriglyceride
pancreatitis
plasmapheresis

Introduction
Hypertriglyceridemia is one of the correctable cause of acute pancreatitis after alcohol consumption and gallstone disease with a reported frequency of 1%-10% of cases of acute pancreatitis.[12] In patients with severe acute pancreatitis, an urgent lowering of Triglyceride is necessary to prevent disease complications and oral pharmacological therapy may not always be feasible.[3] Plasmapheresis is an effective therapeutic option for rapid reduction of serum triglyceride and can be considered early in the management.[45] Here, we present four cases of hypertriglyceride induced pancreatitis with the varied clinical scenarios.
Case Series
A total of four cases of hypertriglyceride-induced pancreatitis who underwent plasmapheresis as a treatment modality for the reduction of serum triglycerides were studied. All four patients didn't have a past history of hyperlipidaemia and acute pancreatitis. Among which two cases were male and two cases were female. Their Mean ages were 41.75yrs, with an age range of 30-55yrs. The baseline characteristics and the outcome of plasmapheresis of the cases are summarized in Table 1.
| CASE 1 | CASE 2 | CASE 3 | CASE 4 | AVERAGE | |
|---|---|---|---|---|---|
| Age | 45 | 37 | 30 | 55 | 41.75 Year |
| Gender | F | M | F | M | - |
| Type 2 Diabetes Mellitus | YES | YES | YES | YES | - |
| Alcohol | NO | NO | NO | NO | - |
| High-Density Lipoproteins (mg/dl) | 24 | 30 | 26 | 27 | 26.75(mg/dl) |
| Cholesterol (mg/dl) | 323 | 368 | 279 | 297 | 316.75(mg/dl) |
| Low-Density Lipoproteins (mg/dl) | 135 | 160 | 145 | 129 | 142.25(mg/dl) |
| Serum Lipase (U/L) | 417 | 2859 | 279 | 2634 | 1547.25(U/L) |
| Triglycerides (mg/dl) | 1359 | 1325 | 1265 | 1718 | 1416.75(mg/dl) |
| Triglycerides After a Plasma Pheresis (mmol/L) | 346 | 310 | 341 | 521 | 379.5(mg/dl) |
| % decrease in Triglycerides After 1st Session of Plasma Pheresis | 74.54% | 76.6% | 73.40% | 69.6% | 73.53% |
| Number of Plasma Pheresis | 1 | 1 | 1 | 2 | 1.25 |
| HbA1C | 9.1 | 8.7 | 10.1 | 9.6 | 9.375 |
| Complication of a Plasma Pheresis | NO | NO | NO | NO | - |
| Severity of Pancreatitis | MSAP | SAP | MSAP | SAP | - |
| APACHE II | 16 | 24 | 16 | 18 | 18.5 |
| Initiation of Symptoms to Initiation of Plasma pheresis | 24HRS | 120HRS | 36HRS | 48HRS | 57HRS |
| Number Of Day in Intensive Care Unit | 2 | 12 | 3 | 4 | 5.25 |
| Number Of Day in Hospital | 5 | 12 | 6 | 8 | 7.75 |
| Serum Creatinine at Admission (mg/dl) | 1.4 | 5.8 | 1.6 | 2.4 | 2.8(mg/dl) |
| Renal replacement therapy Requires | NO | YES | NO | NO | - |
| Triglycerides at Discharge (mg/dl) | 240 | 218 | 242 | 168 | 217(mg/dl) |
| Serun Creatinine at Discharge (mg/dl) | 0.9 | - | 1.0 | 0.8 | - |
| Out Come | Discharge | Death (Sepsis) | Discharge | Discharge | - |
SAP: Severe acute pancreatitis ; MSAP: Moderate Severe acute pancreatitis; HBA1c: Glycalated Haemoglobin; APACHE II: Acute physiology and chronic health evaluation II
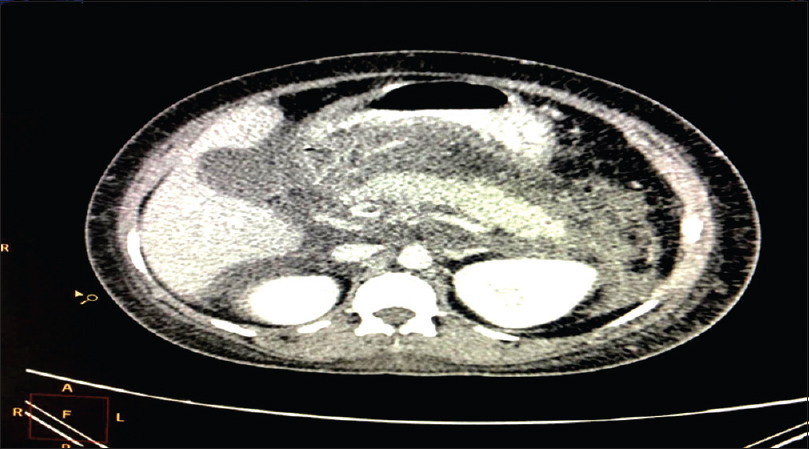
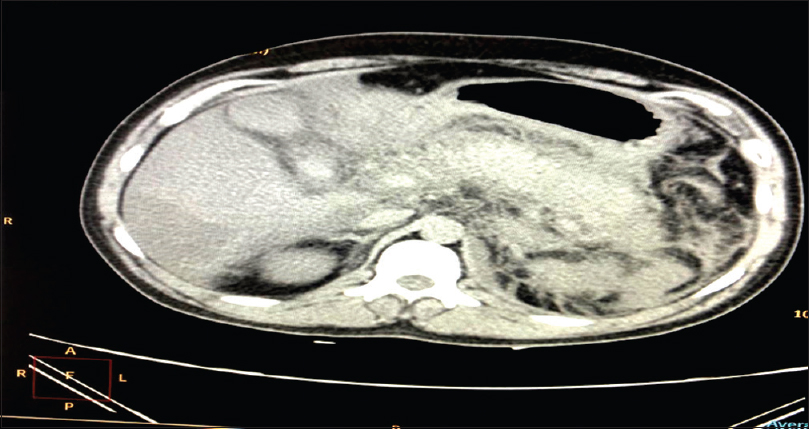
The etiology of Hypertriglyceridemia was secondary to diabetes is all four cases. Two patients has severe and two has moderate pancreatitis by modified Atlanta classification and computed tomography severity index [Figures 1–3]. The mean acute physiology and chronic health evaluation II of patients at the time of admission was 18.5. Mean serum creatinine at the time of admission was 2.8mg/dl (range 1.4-5.8mg/dl). Mean serum lipase and triglyceride at the time of admission was 1547.25U/L and 1416.75mg/dl respectively. All patients showed a significant improvement in triglyceride after plasmapheresis. The mean number of session of Plasmapheresis done was 1.25 (range 1-2). After the first session the mean percentage decrease in triglyceride level was 73.53% (69.6%-76.6%) and mean triglyceride was 379.5mg/dl (Range 310-521mg/dl). After acute control patients were started on lipid-lowering drugs (fibrates). At the time of discharge mean triglyceride of patients were 217mg/dl (Range 168-242mg/dl). None of the patients developed complications related to plasmapheresis. The mean duration of stay in hospitals was 7.75 days with ICU stay was 5.25 days. Three patients were discharge from of hospital and one died due to sepsis. Out of four patients, only one required Renal Replacement therapy. No evidence of gallstone on imaging was noted and patients did not have any endoscopic intervention prior to admission to the hospital for acute pancreatitis. All three patients who were discharged are in follow up with Nephrology and Gastroenterology department, having a normal renal parameter.

- CT scan of abdomen of Case 1
- CT scan of abdomen of Case 2
- CT scan of abdomen of Case 3
Discussion
The association between acute pancreatitis and hyperlipidaemia is well known, both as a precipitant and as an epiphenomenon [6]. The exact pathophysiology of hypertriglyceride-induced acute pancreatitis is not clear. A proposed mechanism is the hydrolysis of triglyceride by pancreatic lipase, leading to accumulation of high concentration of free fatty acids and chylomicrons which can produce acinar cell injury and capillary plugging causing ischemia and acidosis activating trypsinogen and acute pancreatitis [7].
The management of patients with hypertriglyceridemia-induced pancreatitis includes treatment of acute pancreatitis and the reduction of serum triglyceride levels with the goal of preventing necrotizing pancreatitis and organ failure. The main treatment modalities for reduction of hypertriglycerides are insulin and apheresis.
Many insulin regimens have been reported to lower triglyceride levels to less than 500mg/dl over 3.5 to 4 days [89].
Plasmapheresis is an effective therapeutic option for hypertriglycerides induced severe acute pancreatitis with a rapid reduction of serum triglyceride and can be considered early in the management [45]. The absolute indications of plasmapheresis in patients with hypertriglyceridemia are (a) patient refractory to nutritional and pharmacological approaches,(b) serum triglyceride exceed 1000mg/dl,(c) worsening inflammation and organ dysfunction [10]. The relative indications include (a) serum lipase 3 times the upper limit of normal, (b) severe hypocalcaemia, and (c) Lactic acidosis. Our patients had triglycerides >1000mg/dl with Severe Acute pancreatitis with lipase >3 times.
The beneficial effect of plasmapheresis is believed to be because of rapid decrease in triglyceride levels; however, removal of excessive proteases from the plasma which are key enzymes in inflammation and replacement of consumed protease inhibitors might be additional benefit [7].
Plasmapheresis involves removal of 1-1.5volume of plasma through centrifugation or filtration under transient anticoagulation and replacing it by 5% human albumin or fresh frozen plasma. Plasmapheresis is relatively a safe procedure with few complication [11]. Our patients did not experience any adverse event during the plasmapheresis procedure. Studies comparing plasmapheresis replacement fluid (albumin versus fresh frozen plasma) in patients with hypertriglyceride induced pancreatitis are lacking. Our patients received heparin as an anticoagulant and 5% albumin as replacement fluid with two unit of fresh frozen plasma at the end of plasmapheresis.
Maximal reduction in morbidity and mortality can be achieved when patients undergo plasmapheresis as early as possible. According to kyriakidis et al. plasmapheresis should be performed as early as possible within the first 48hr to prevent irreversible organ damage and prevent further attacks of pancreatitis [12]. Out of 4 in 3 patients, plasmapheresis was done within 48hr and the patient was relieved of acute symptoms following the session of plasmapheresis. The patients who received plasmapheresis after 48hrs showed poor prognosis.
In our study, plasmapheresis was done in view of severe hypertriglycedemia and a single session of plasmapheresis reduced triglyceride level by 73.45%, which was higher than reduction (61-70%) shown in similar studies [13].
Gubensek et al.[3] observed a mean reduction of 59% in triglyceride levels with plasmapheresis as compared to 27% with conservative management over 24hr, which was significantly lower than the reduction by plasmapheresis and concluded that plasmapheresis effectively reduced triglyceride levels at a faster rate than the conservative treatment and is associated with a low rate of complications.
Triglyceride levels were reduced to 217 mg/dl after plasmapheresis. No further plasmapheresis was performed and the patient was managed conservatively in accordance with the study of Ewald and kloer [14] which states that plasmapheresis should be performed until Triglyceride levels have been lowered to 500 mg/dl.
Conclusion
Hypertriglyceridemia is a common clinical problem, and if markedly elevated, can lead to pancreatitis. Pancreatitis in the setting of diabetes and severe hypertriglyceridemia is often underdiagnosed disease with significant morbidity and an increased risk of mortality. When suspected, prompt diagnosis and treatment should be initiated by supportive therapy, lowering blood glucose levels and rapid reduction of triglyceride levels. Plasmapheresis is an effective and rapid measure for the reduction of triglyceride level below 500mg/dl. The limitation of plasmapheresis is its cost and availability in all medical centers. The benefit of plasmapheresis in reducing the hospital stay and less frequent monitoring of patients triglyceride and glucose levels need to be considered. A need for randomised controlled trail comparing insulin use and plasmapheresis to lower triglyceride levels with a good sample size is required to establish the benefit of each of them.
Financial support and sponsorship
Nil
Conflict of interest
There are no conflicts of interest
References
- [Acute hypertrygliceridemic pancreatitis] Gastroenterol Hepatol. 2013;36(4):274-9. Spanish
- [Google Scholar]
- Current knowledge of hypertriglyceridemic pancreatitis. Eur J Intern Med. 2014;25(8):68994.
- [Google Scholar]
- Factors affecting outcome in acute hypertriglyceridemic pancreatitis treated with plasma exchange: An observational cohort study. PLoS One. 2014;9(7):e102748.
- [Google Scholar]
- Plasmapheresis as treatment for hyperlipidemic pancreatitis. Eur J Intern Med. 2014;25:160-3.
- [Google Scholar]
- Plasmapheresis in the treatment of hypertriglyceridemia. Orv Hetil. 2014;155:1203-6.
- [Google Scholar]
- Treatment of severe hypertriglyceridemia in nondiabetic patients with insulin. Am J Emerg Med. 2005;23:415.
- [Google Scholar]
- [Insulin therapy in patients with severe hypertriglyceridemia] Rev Med Inst Mex Seguro Soc. 2006;44:235.
- [Google Scholar]
- Severe hypertriglyceridemia induced pancreatitis in pregnancy. Case Rep Obstet Gynecol. 2014;2014:485493.
- [Google Scholar]
- Predictors of complications in therapeutic plasma exchange. J Clin Apher. 2009;24:225-31.
- [Google Scholar]
- Plasmapheresis in the treatment of hypertriglyceridemia-induced pancreatitis: A community hospital's experience. J Clin Apher. 2010;25:229-34.
- [Google Scholar]
- Treatment options for severe hypertriglyceridemia (SHTG): The role of apheresis. Clin Res Cardiol Suppl. 2012;7(Suppl 1):31-35.
- [Google Scholar]




