

Translate this page into:
IgA dominant postinfectious glomerulonephritis: Report of two cases
Address for correspondence: Dr. V. Rajakumar, Department of Nephrology, Government Stanley Hospital, Chennai - 600 001, Tamil Nadu, India. E-mail: drrajmd78@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Immunoglobulin A (IgA) dominant postinfectious glomerulonephritis (IgA PIGN) is a distinct clinical entity increasingly recognized in adult. It usually presents with reduced glomerular filtration rate, heavy proteinuria, and has unfavorable prognosis. Immunofluorescence study of renal biopsy specimens have IgA as dominant or codominant antibody. We encountered two cases of IgA dominant PIGN recently presenting as rapidly progr essive glomerulonephritis and managed conservatively. Both the patients are on follow-up and do not have complete recovery of renal function till date. Long-term follow-up is needed to assess the progression of the disease in these patients.
Keywords
Heavy proteinuria
immunoglobulin A dominant postinfectious glomerulonephritis
severe renal failure
unfavorable prognosis

Introduction
Acute postinfectious glomerulonephritis (APIGN) is an immune complex glomerulonephritis that most commonly affects children following Streptococcal upper respiratory tract or skin infections.[12] Over recent years, the spectrum of the disease has been changed. Other sites of infection including skin, other organisms particularly Staphylococcus and gram negative bacteria and increased incidence in adults are reported frequently.[345]
Immunoglobulin dominant PIGN (IgA PIGN) is characterized by diffuse endocapillary proliferative glomerulonephritis on light microscopy (LM), IgA as the dominant or codominant immunoglobulin on immunofluorescence (IF), along with subepithelial ‘hump’ shaped electron dense deposits on electron microscopy (EM).[6] It usually manifests as acute or rapidly progressive renal failure, proteinuria often severe, and more than 80% of cases have persistent renal dysfunction.[7]
Case Reports
Case 1
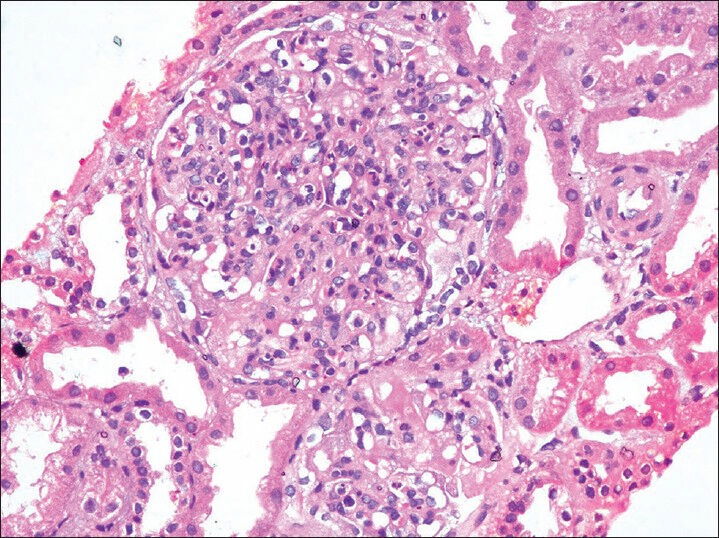
A 30-year-old lady with diabetes and hypertension on treatment for 2 years, was admitted with complaints of facial puffiness and swelling of legs for 2 weeks. On clinical examination, she had pedal edema, hypertension, and no evidence of diabetic retinopathy. Urinalysis showed protein 3+ and blood 3+. Investigations showed a hemoglobin of 9.9 mg/dl, white blood cell (WBC) count 8,700/mm3(polymorphs 55%, lymphocytes 24%, and others 1%), platelets 2.89 lakhs/mm3, and serum creatinine progressed from 2.7 to 4 mg/dl over a period of 7 days. Serology showed hepatitis B surface antigen (HBsAg), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) negative; complements C3 60 mg/dl (79-152 mg/dl) and C4 21 mg/dl (16-38 mg/dl); and antistreptolysin O (ASO) and antinuclear antibody (ANA) were negative. Blood culture showed no growth. Renal biopsy was done; LM showed 13 glomeruli out of which seven globally sclerosed; fibrocellular crescents in three glomeruli; remaining glomeruli showed endocapillary proliferation with neutrophilic infiltration; and few inflammatory interstitial infiltrate seen. Arteries showed fibrous intimal proliferation [Figure 1]. IF showed +3 coarse granular positivity for C3 and IgA over the mesangium and capillary walls with higher intensity of staining for C3 than IgA. Staining for IgM, IgG, and C1q were negative [Figures 2 and 3].

- Segmental endocapillary proliferation (H and E, ×40)

- Intense (+3) coarse granular positivity for C3 along the capillary walls (immunofluorescence, ×20)

- Coarse granular positivity (+3) for immunoglobulin A (IgA) along the capillary walls (IF, ×40)
Case 2
A 37-year-old gentleman was admitted with oliguria, swelling of legs, and breathlessness for 10 days; preceded by upper respiratory tract infection 1 week back. On clinical examination, he had pedal edema and hypertension. Urinalysis showed protein 3+ and blood 3+ and urine spot protein/creatinine ratio (PCR) 7.89. Investigations showed a hemoglobin of 9 gm/dl, WBC count 5,500/mm3(polymorphs 61%, lymphocytes 33%, and others 6%), platelets 3 lakhs/mm3, and serum creatinine progressed from 1.1 to 4.3 mg/dl over a period of 8 days. Serology showed HBsAg, HCV, and HIV negative; complements C3 39.7 mg/dl (79-152 mg/dl) and C4 17.1 mg/dl (16-38 mg/dl); ASO positive; and ANA negative. Blood culture showed no growth. Renal biopsy was done; LM showed 14 glomeruli, all with global endocapillary proliferation with neutrophilic infiltration; partial cellular crescents in four glomeruli; patchy interstitial inflammatory infiltrate; normal vessels [Figure 4]. IF showed +3 coarse granular positivity for C3 over the mesangium and capillary walls with weaker (+1) positivity of IgA and IgM. Staining for IgG and C1q were negative [Figures 5 and 6].
- Global endocapillary proliferation (H and E, ×40)

- Intense (+3) coarse granular positivity for C3 along the capillary walls (IF, ×20)

- Weaker (+1) positivity for IgA along the capillary walls (IF, ×40)
In both cases causative organism could not be established and both were managed conservatively. Steroids were not used. Over a period of 10 months follow-up, the first case has persistent renal dysfunction (serum creatinine 3.6) and persistent proteinuria; whereas, the second case has partial recovery of renal dysfunction (serum creatinine 1.6) and nephrotic proteinuria (urine spot PCR 6.3) after a period of 3 months follow-up.
Discussion
IgA PIGN is an increasingly recognized morphologic variant of APIGN, particularly in the elderly. In contrast to classic APIGN, which has typical glomerular deposition of IgG and C3 or C3 only, IgA is the sole or dominant immunoglobulin in IgA PIGN.[7] So far, fewer than hundred cases of IgA PIGN have been reported in literature.[8]
Here we presented two cases of biopsy proven IgA APIGN. Both of them are below 60 years. In other studies, average age at diagnosis is 60 years (range 16-85 years).[6789101112] One of our patients is a diabetic. Previous studies reported that IgA PIGN was mainly associated with diabetes mellitus.[678] One of our patients had upper respiratory tract infection and the causative organism could not be established in both. Previous case studies revealed that Staphylococcus and gram negative organisms are the most frequent organisms associated within IgA PIGN. Pharyngitis is superceded by infections of skin, urinary tract, and lung.[578111314]
Both the patients presented with severe renal failure, overt proteinuria, and hypertension; and one had nephrotic proteinuria. The average peak serum creatinine of our cases is 4.15 mg/dl. In other case reports average peak serum creatinine was 4 mg/dl and 51% of the patients had nephrotic proteinuria (range: 0.15-15 g/day).[789] Hypocomplementemia noted in both of our patients. In other studies only 69% of patients had low complement levels.[78]
LM of renal biopsy of both patients showed the typical endocapillary proliferative GN. Other reports showed only 63% patients had typical picture and 30% had mesangial proliferation.[678910111213] IF study revealed IgA as dominant and codominant antibody and higher intensity for complement 3 than IgA, the classical picture reported in other studies.[678910111213]
Both of our patients were treated with antibiotics only. Till date, there is no systematic evaluation of treatment options and their effectiveness in the treatment of IgA PIGN including steroids.[715]
In our report both the patients are in follow-up for a short period (<1 year) and both had partial recovery of renal failure and persistent proteinuria. Long-time follow-up is needed to assess the progression of the disease in our cases. Nasr et al., in his review noted that only 16% of IgA APIGN had full recovery of renal function (≤1.2 mg/dl) whereas 43% had persistent renal dysfunction and 41% progressed to end-stage renal disease (ESRD).[7] The prognosis of IgA PIGN is less favorable than that of typical APIGN.[678910111213]
The mechanism of selective IgA deposition in IgA PIGN is unclear. It may be related to increased serum levels of IgA and IgA-containing circulating immune complexes, possibly as a result of subclinical mucosal infection or decreased IgA hepatic clearance caused by serum IgA1 hypersialylation especially in diabetics.[1617] Koyama et al., found that patients with methicillin resistant Staphylococcus aureus (MRSA)-associated glomerulonephritis had polyclonal increases of serum IgA and IgG, high levels of circulating immune complexes. Staphylococcal enterotoxin, acts as a superantigen which bypass normal antigen presentation by binding directly to the major histocompatibility class II molecules on antigen-presenting cells and to the variable portion of the beta chain of T cells leading to massive T cell activation and production of high amounts of proinflammatory cytokines.[13]
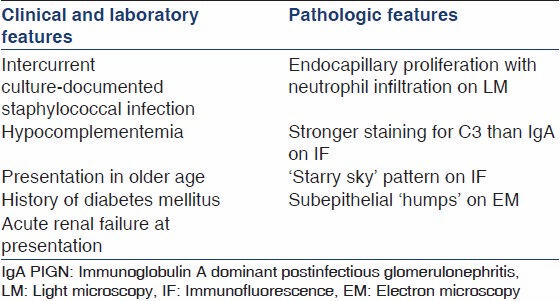
The type of IgA in IgA PIGN is unknown and it remains to be determined whether these patients have aberrant IgA molecule glycosylation as in IgA nephropathy. Importantly, IgA dominant PIGN need to be distinguished from IgA nephropathy[710] [Table 1].
Conclusions
IgA APIGN is an increasingly recognized entity in adults commonly associated with Staphylococcus and gram negative organisms. It commonly affects diabetics through diverse routes of infection predominantly the skin and has worse prognosis when compared with classical APIGN. Greater awareness among nephrologists and nephropathologists is needed to recognize this rare but serious entity and to differentiate it from more common IgA nephropathy.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Atlas of nontumor pathology: Non-neoplastic kidney diseases. Washington: American registry of pathology-Armed Forces Institute of Pathology; 2005.
- Acute postinfectious glomerulonephritis and glomerulonephritis caused by persistent bacterial infection. In: Jennette JC, Olson JL, Schwartz MM, Silva FG, eds. Heptinstall's Pathology of the Kidney (6th ed). Philadelphia: Lippincott Williams and Wilkins; 2007.
- [Google Scholar]
- Postinfectious glomerulonephritis in the elderly. J Am Soc Nephrol. 2011;22:187-95.
- [Google Scholar]
- Acute postinfectious glomerulonephritis in the modern era: Experience with 86 adults and review of the literature. Medicine. 2008;87:21-32.
- [Google Scholar]
- The current spectrum of infectious glomerulonephritis: Experience with 76 patients and review of the literature. Medicine. 1995;74:63-73.
- [Google Scholar]
- IgA-dominant acute post staphylococcal glomerulonephritis complicating diabetic nephropathy. Hum Pathol. 2003;34:1235-41.
- [Google Scholar]
- IgA-dominant postinfectious glomerulonephritis: A new twist on an old disease. Nephron Clin Pract. 2011;119:c18-25.
- [Google Scholar]
- Clinicopathologic Features of IgA-Dominant Postinfectious Glomerulonephritis. Korean J Pathol. 2012;46:105-14.
- [Google Scholar]
- IgA-dominant postinfectious glomerulonephritis: A report of 13 cases with common ultrastructural features. Hum Pathol. 2008;39:1309-16.
- [Google Scholar]
- Discrimination between postinfectious IgA-dominant glomerulonephritis and idiopathic IgA nephropathy. Ren Fail. 2010;32:572-7.
- [Google Scholar]
- Immunoglobulin A-dominant postinfectious glomerulonephritis: Frequent occurrence in nondiabetic patients with Staphylococcus aureus infection. Hum Pathol. 2011;42:279-84.
- [Google Scholar]
- Glomerulonephritis and Staphylococcal aureus infections. Clin Nephrol. 1980;14:256-61.
- [Google Scholar]
- Glomerulonephritis associated with MRSA infection: A possible role of bacterial superantigen. Kidney Int. 1995;47:207-16.
- [Google Scholar]
- Glomerulonephritis induced by methicillin-sensitive Staphylococcus aureus infection. Clin Exp Nephrol. 2003;7:247-9.
- [Google Scholar]
- Successful treatment of post-MRSA infection glomerulonephritis with steroid therapy. Clin Nephrol. 2008;70:344-7.
- [Google Scholar]
- Hypersialylated macromolecular serum immunoglobulin A1 in type 2 diabetes mellitus. Clin Biochem. 2001;34:35-41.
- [Google Scholar]
- Elevation of serum IgA1 levels in patients with diabetic nephropathy. Nephron. 1993;63:355.
- [Google Scholar]




