

Translate this page into:
IgA dominant poststaphylococcal glomerulonephritis: Complete recovery with steroid therapy
Address for correspondence: Dr. M. Eswarappa, Department of Nephrology, M.S. Ramaiah Medical College, M.S.R.I.T. Post, M.S.R. Nagar, Bengaluru - 560 054, Karnataka, India. E-mail: manasnephro2002@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
A 70-year-old diabetic male presented with pedal edema, breathlessness, nausea, vomiting and reduction in urine output for 4 days. About 6 weeks earlier he had an episode of staphylococcal pneumonia, which resolved with antibiotics. Physical examination revealed stable vitals, bilateral pitting pedal edema and bilateral basal crackles. No signs of active infection were noted. Initial labs were remarkable for serum creatinine (SCr) of 9.03 mg/dl, blood urea nitrogen of 87 mg/dl, total leukocyte count of 11,580/cumm, hemoglobin of 11.65 g/dl and platelet count of 247,620/cumm. Baseline renal function tests 6 weeks earlier were within the normal limits. Urinalysis revealed 8-10 leukocytes/high power field, numerous red blood cells (RBCs), dysmorphic RBCs, protein 2+, glucose 1+, 24 h urine protein was 4.07 g. Blood cultures were negative. Abdominal ultrasound revealed kidneys of normal size with grade 1 bilateral nephropathy. Serological tests such as antinuclear antibodies, antineutrophil cytoplasmic antibody, anti-streptolysin O, anti-glomerular basement membrane, human immunodeficiency virus, hepatitis B, hepatitis C and syphilis were negative. Complement levels were at the lower limit of normal. Renal biopsy revealed cellular epithelial crescents involving about 25% glomeruli, marked endocapillary proliferation, neutrophilic infiltration, increased mesangial matrix and cellularity. Immunofluorescence revealed coarse granular positivity for IgA and C3 along capillary loops and mesangium [Figure 1]. Clinicopathological findings were consistent with IgA dominant PIGN.[12]
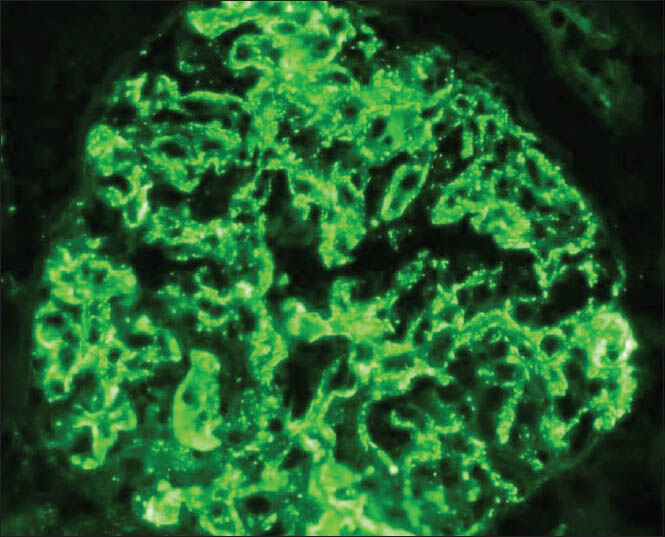
- Immunofluorescence showing coarse granular positivity for IgA(+++) along the capillary loops and in the mesangium (starry sky pattern)
He was initiated on pulse intravenous methyl prednisolone in addition to symptomatic treatment, followed by tapering dose of oral prednisone. His SCr peaked at 10.29 mg/dl. He required multiple sessions of intermittent hemodialysis during hospital stay. His SCr after 3 months, improved to 1.2 mg/dl, estimated glomerular filtration rate of 63.6 ml/min/1.73 m2. No recurrence of staphylococcal infection was observed.
IgA dominant PIGN is a relatively new entity.[123] It is usually associated with staphylococcal infection involving heterogeneous sites, elderly age and diabetes. Peak SCr values range from 1.4 to 14.5 mg/dl. Proteinuria ranges from 0.15 to 15 g/day with 51% of patients have nephrotic range proteinuria.[1] Most common histologic pattern is endocapillary proliferative and exudative glomerulonephritis (GN), along with IgA and C3 deposition in glomeruli.[12]
It is an important differential to consider in patients presenting with rapidly progressive GN. Distinction needs to be made from IgA nephropathy, C3 glomerulonephritis, Henoch-Schönlein purpura.[134] Prognosis is usually poor. Independent poor prognostic factors include older age, higher SCr, tubulointestinal scarring, underlying comorbidities.[3] In one study, complete recovery of renal function defined as SCr ≤ 1.2 mg/dl was observed in only 16% of patients, while 41% of patients progressed to end stage renal disease.[1] It has been previously noted that steroids may have a role in patients who fail to respond to antibiotic therapy alone and in crescentic forms of PIGN.[5] Our patient, who achieved complete renal recovery despite elderly age, diabetes, crescentic changes, high SCr, emphasizes that steroids might be beneficial in the absence of active infection. Given the significant benefit of alleviating need for long-term hemodialysis, further studies are required to provide recommendations regarding role of steroids.
References
- IgA-dominant postinfectious glomerulonephritis: A new twist on an old disease. Nephron Clin Pract. 2011;119:c18-25.
- [Google Scholar]
- Clinicopathologic features of IgA-dominant postinfectious glomerulonephritis. Korean J Pathol. 2012;46:105-14.
- [Google Scholar]
- Bacterial infection-related glomerulonephritis in adults. Kidney Int. 2013;83:792-803.
- [Google Scholar]
- Discrimination between postinfectious IgA-dominant glomerulonephritis and idiopathic IgA nephropathy. Ren Fail. 2010;32:572-7.
- [Google Scholar]
- Postinfectious glomerulonephritis: Is there a role for steroids? Indian J Nephrol. 2011;21:116-9.
- [Google Scholar]




