

Translate this page into:
Malignant hypertension and nephrotic range proteinuria without hematuria: IgA nephropathy
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
A 39-year-old male was admitted with generalized headache, vomiting, and sudden onset blurring of vision. There was no history of hypertension, fever, altered sensorium or convulsion. On examination, the patient had dyspnea, mild pallor, tachycardia and a blood pressure (BP) of 210/110 mm of Hg. Ophthalmoscopy revealed bilateral papilledema with macular star and flame shaped hemorrhage in right eye and soft exudates in the left eye. The hypertensive emergency was managed with intravenous Labetelol. Investigations revealed anemia (Hb: 10.0 g/dl), dysmorphic red cells on peripheral blood smear, serum creatinine: 4.0 mg/dl, normal serum electrolytes except hypocalcemia (7.3 mg/dl). Urinalysis showed albuminuria (+++) without any evidence of microscopic hematuria. His 24 h urinary protein excretion was 4.68 g. Serum albumin level was 3.0 g/dl. Serum thyroid stimulating hormone level (3.5 mIU/L) and urinary metanephrine (3.5 ×mol/24 h) levels were normal. Collagen vascular disease and vasculitis were excluded. Ultrasonography of abdomen showed bilateral renal parenchymal disease (right kidney: 85 mm, left kidney: 92 mm). Renal artery Doppler study was normal. The patient was treated with ramipril, amplodipine and prazosin for control of BP.
Renal biopsy [Figure 1] showed IgA nephropathy (M1, S1, E0, T2, global glomerulosclerosis: 7/12 glomeruli, fibrocellular crescents: 2/12 glomeruli). The sections were stained for IgG, IgM, IgA, C3, C1q, Kappa and Lambda light chains [Figure 2]. There was + 3 mesangial positivity for IgA. Stains for IgG, IgM, C3 and C1q were negative. Sections and special stains (PAS, silver and trichrome) include renal cortical tissue.

- Light microscopic description of renal biopy samples stained with special stain (PAS, silver and trichrome). Twelve glomeruli are included in this biopsy of which 7 are globally sclerotic. Segmental sclerosis with adhesion to the Bowmans capsule are identified in 3 glomeruli. Fibrocellular crescent is present in two glomeruli. All the glomeruli show an increase in cellularity and mesangial matrix. Interstitial fibrosis, tubular atrophy and tubular loss involves more than 50% of the core. There is arteriolar hyalinosis and fibrointimal proliferation of the arteries
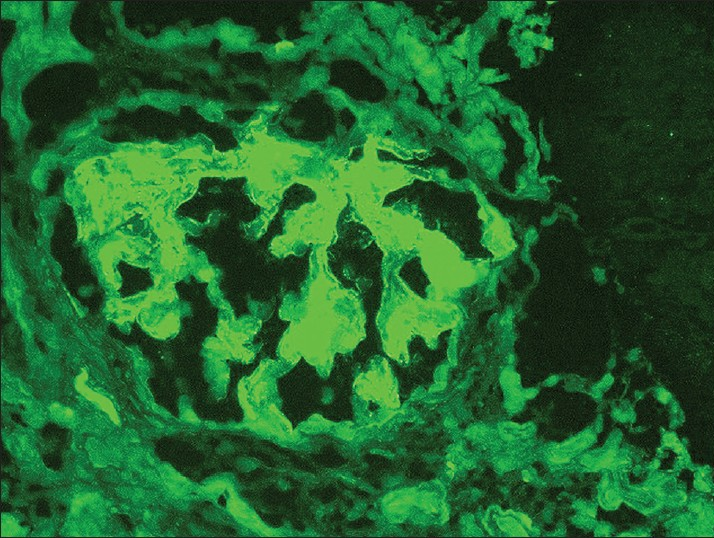
- Imunofluorescence staining of the renal biopsy samples: 4 glomeruli are present for evaluation. The sections are stained for IgG, IgM, IgA, C3, C1q, Kappa & Lambda light chains. There is +3mesangial positivity for IgA. Stains for IgG, IgM, C3 and C1q are negative
IgA nephropathy (IgAN) constitutes between 7% and 16% of biopsy samples from India (average 8%).[12] It classically presents as episodic macroscopic hematuria following upper respiratory tract infection or asymptomatic proteinuia with microscopic hematuria in young male. Malignant hypertension is a rare presenting feature.[3] In our patient, malignant hypertension was the presenting feature. Other exceptional features were normoalbuminemia and absence of oedema in the face of nephrotic range of proteinuria and absence of hematuria.
Among patients with nephrotic- range proteinuria, normoalbuminaemia was associated with IgA N with very high specificity. It is possibly due to lower proportion of albumin in urinary protein (66%) and normal capillary permeability in patients with IgAN.[4] Our patient also had a lower urinary albumin to protein ratio (53%). The most striking finding in our patient was proteinuria without microscopic hematuria. This finding is classically not described in IgAN. However, in a Finnish cohort, 5.8%of biopsy proven IgAN patients had proteinuria without microscopic haematuria.[5]
References
- Primary IgA nephropathy in north India: Is it different? Postgrad Med J. 2012;88:15-20.
- [Google Scholar]
- Normoalbuminaemia is associated with IgA nephropathy in primary glomerulopathy with nephrotic-range proteinuria in Chinese patients. Nephrol Dial Transplant. 2011;26:1247-52.
- [Google Scholar]
- Polymorphism of the cytokine genes and IgA nephropathy. Kidney Int. 2002;61:1079-85.
- [Google Scholar]




