

Translate this page into:
Periodontal status in patients undergoing hemodialysis
Address for correspondence: Dr. Parkar Sujal M, B-25 Krishna Bunglows, Gandhinagar Highway, Motera, Ahmedabad- 380 005, Gujarat, India. E-mail: drsujal_pcd@live.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The aim of the study was to assess the periodontal status of patients among group of patients receiving hemodialysis in two super specialty renal institutes in the state of Gujarat. A cross-sectional study of 304 subjects, 152 subjects each in dialysis, and control group was conducted. Oral hygiene status was assessed using a Simplified Oral Hygiene Index, and periodontal status was assessed using the Community Periodontal Index (CPI) and Loss of Attachment (LOA) as per WHO methodology 1997. The dialysis group had poor oral hygiene than the control group (P<0.001). There was high severity of periodontitis in the dialysis group as compared with the control group (P<0.001). None of the subjects had healthy periodontium. There was high severity of periodontitis (for both in terms of CPI and LOA) in the dialysis group as compared with control group that was found to be statistically highly significant (P<0.001). However, no statistically significant difference was observed (P>0.05) when the intergroup comparison for CPI and LOA were made among the subgroups according to the duration of dialysis. Periodontal disease is prevalent in chronic renal failure patients who showed the unacceptable level of oral hygiene and hence there is need for oral health promotion and preventive programs among the patients receiving dialysis.
Keywords
Chronic kidney disease
hemodialysis
oral health
periodontitis
renal failure

Introduction
Renal failure is a process that expresses a loss of functional capacity of the structure and functional unit of kidneys–nephrons. Chronic renal failure (CRF) is defined as a progressive decline in the renal function associated with a reduced glomerular filtration rate (GFR). Loss of renal function results in accumulation of metabolic waste product affecting various organs of the body.[12] Today, renal transplantation is the treatment of choice for patients with the chronic renal failure. However, the use of transplantation is limited by organ availability.[13] In the last 3 to 4 decades, improvements in dialysis have reduced morbidity and mortality among patients with chronic renal disease.[4]
Patients presenting with CRF are at high risk of developing oral health complications, such as narrowing of pulp chamber, enamel abnormalities, xerostomia, premature tooth loss, increased prevalence of calculus, and periodontal disease, when compared to the general population.[24–6] Since CRF exhibit unique present medical, psychological, and socio-economical characteristics that may predispose to odontological problems, oral health in dialysis and transplant patients has been proposed to be poor, with a potential impact on patient's morbidity, mortality, and quality of life.[6] Specific effects of chronic renal disease and renal replacement therapy on periodontal tissues include gingival hyperplasia in immune suppressed renal transplantation patients and increased levels of plaque, calculus, and possible increased prevalence and severity of gingivitis and destructive periodontal diseases in CRF patients on dialysis maintenance therapy.[7]
Only a few studies performed in a limited number of patients reported periodontal health status in CKD patients,[2489] and no reports of periodontal health status of CRF performed in Gujarat, India. Moreover, comparison of the periodontal status between dialysis patients and healthy individuals has not been described so far. Therefore, the purpose of this study was to assess the oral health status and periodontal status among group of patients receiving renal dialysis.
Patients and Methods
Study subjects
The cross-sectional study was conducted among two groups: patients with CRF (dialysis group) and healthy subjects (control group) attending the Institute of Kidney Disease and Research Centre, Ahmedabad and Muljibhai Patel Urological Hospital, Nadiad, Gujarat, India. The CRF patients were matched with control group to age and gender. These subjects were the relatives of the patients with CRF attending the dialysis unit at Institute of Kidney Disease and Research Centre, Civil Hospital Campus, Ahmedabad and Muljibhai Patel Urological Hospital, Nadiad, Gujarat, India. A total of 152 subjects in each group; 114 (75%) male and 32 (25%) female subjects were included in the study. The mean ages were 37.33±11.86 and 37.25±11.93 years for dialysis and control group, respectively. All participants gave informed consent to participate in this study, which was approved by ethical committee of Sumandeep Vidyapeeth, Vadodara, Gujarat, India.
Clinical examination and indices
The periodontal examination of the dialysis patients was done at the dialysis center of both the institutes. The medical data were retrieved from patient files. All periodontal examinations were done by the same dentist (PSM.). The examiner could not be “blinded” to the subject's general condition, since they were examined in a hospital. The examiner had been calibrated for periodontal assessment by a senior (ACG). The clinical examination was carried out in artificial light with the use of a plane mouth mirror and WHO periodontal probe.
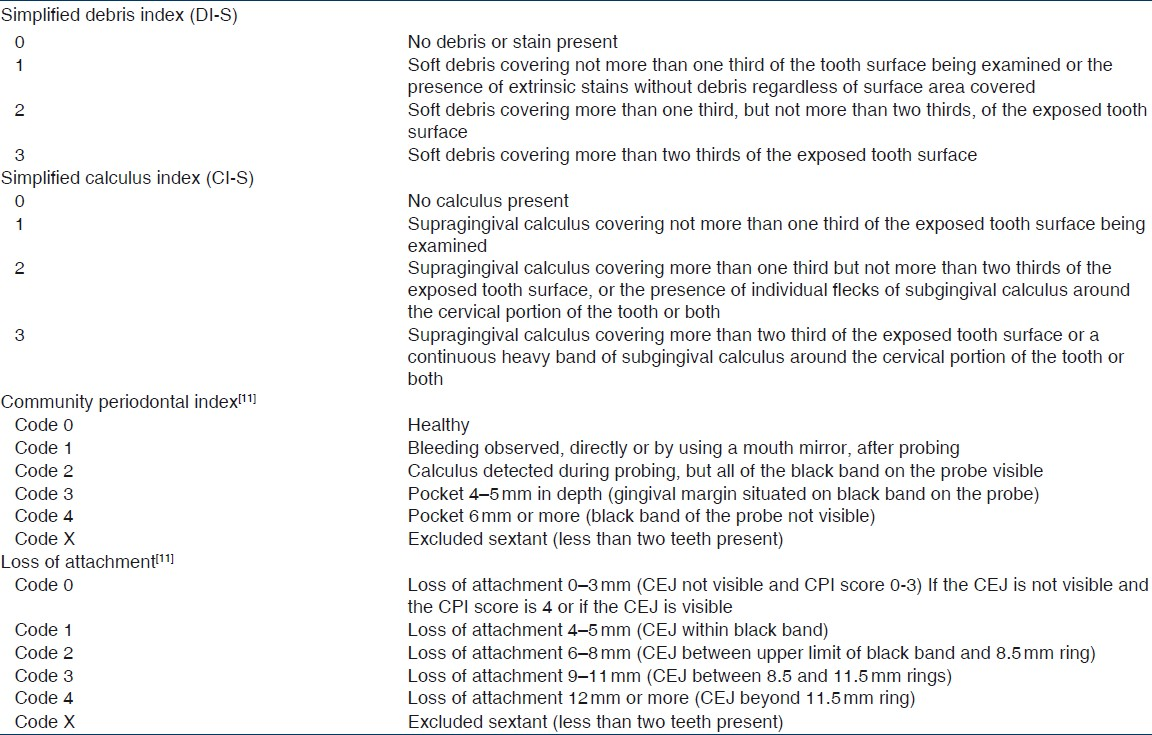
After explaining the study design to the participants, the oral hygiene status was assessed by Simplified Oral Hygiene Index (Greene and Vermillion, 1964)[10] on six indexed teeth (16-upper right posterior first molar, 11-upper right central incisor, 26-upper left posterior first molar, 36-lower left posterior first molar, 31-lower left central incisor, and 46-lower right posterior first molar) and the periodontal status was assessed by Community Periodontal Index (CPI) and Loss of Attachment (LOA) as per WHO methodology 1997 (World Health Organization Oral Health Surveys – Basic methods, 1997),[11] the same indexed teeth were examined. The description of dental indices is presented in Table 1.
In order to determine the effect of the duration of hemodialysis on clinical periodontal status, the dialysis group was further divided into four subgroups: (1) those that have been on dialysis for less than 3 months, (2) those that have been on dialysis for 4–6 months, (3) those that have been on dialysis for 7–9 months, and (4) those that have been on dialysis for 10–12 months.
Student t-test was used to analyze the difference between the means of the two groups regarding clinical parameters. The Chi square test was used to analyze difference between the proportions of the two groups. One-way analysis of variance (ANOVA) was used to determine the difference in clinical parameters among the subgroups. The tests were two-sided, and P values <0.05 were considered significant. Data were analyzed using SPSS statistical package version 17 (SPSS Inc., Chicago, III, USA).[12]
Results
Oral hygiene status (OHI-S)
The simplified oral hygiene index revealed that only 14 (9.21%) dialysis patients had good oral hygiene with mean score of 0.77±0.29, while in control group 55 (36.18%) subjects had good oral hygiene with mean score of 0.76±0.25. This difference observed was statistically not significant (P=0.89). One hundred twelve (73.68%) subjects had fair oral hygiene in the dialysis group while 94 (61.84%) subjects had fair oral hygiene in the control group. The mean scores are 2.05±0.49 and 1.79±0.55, respectively. This difference observed was statistically significant (P<0.001). 26 (17.11%) subjects had poor oral hygiene in dialysis group while three (1.97%) subjects had poor oral hygiene in control group. The mean scores are 3.95±0.63 and 3.27±0.19, respectively. This difference observed was statistically not significant (P=0.07) [Table 2].

Community periodontal index
The highest CPI code was used to assess the periodontal status in both dialysis and control group. 51.97% (n=79) of subjects had 4–5 mm pocket depth (Code 3), as compared to 15.13% (n=23) in the control group. On the other hand, 43.42% (n=66) of patients had calculus and plaque retentive factors (Code 2) in the dialysis group, whereas in the control group 77.63% (n=118) had calculus and plaque retentive factors (Code2). None of the subjects had score Code 0. This difference observed was statistically significant (P<0.001) [Table 3].

Loss of attachment
The highest LOA code was used to assess the periodontal status in both dialysis and control group. 59.21% (n = 90) of subjects had 0–3mm loss of attachment (Code 0) followed by 36.18% (n = 55) had 4–5mm loss of attachment (Code1) in the dialysis group. In the case of the control group 95.39% (n = 145) subjects had 0–3mm loss of attachment (Code 0) followed by 4.61% (n = 7) had 4–5 mm loss of attachment (Code1). None of the subjects had Code 3 and Code 4 score in both the groups. This difference was statistically significant (P<0.001) [Table 3].
The association between duration of hemodialysis and the periodontal status among the patients was analyzed; however, no significant associations were found for any of the scores [Table 4].

Discussion
This study was conducted among 304 study subjects – 152 for dialysis group and 152 for control group. The dialysis group was matched with the control group in age and gender. The relatives of the patients receiving dialysis formed the control group. This approach is clinically justified in relation to the specific population of dialysis patients, and likely more reliable in view of their unusual accumulation of risk factors for periodontal disease.[24] The dialysis group was further divided into four subgroups based on the duration of dialysis to see if the duration of hemodialysis had any effect on periodontal health. As per the medical protocol of both the institutes, if the patients conditions was not improved within 1-year duration of dialysis than such patients were referred for renal transplantation for its further management. Since, the aim of this study was to assess the periodontal status among patients receiving renal dialysis rather than for renal transplantation so; the patients receiving dialysis for more than 1-year duration were excluded in this study.
Age is the known risk factor for both chronic kidney diseases[1314] as well as periodontal diseases.[15] The mean age of the dialysis patients in the present study was 37.33±12.76 years, which was found to be lower than subjects of previous studies.[916–21] The mean age of the dialysis patients in this study was higher in this study than the subjects of Davidovich et al.[2] and Al Wahadni A.[22]
There was significant difference between the dialysis and control group in terms of oral hygiene status. This result was in agreement with previous results reported.[9161823] This difference might be due to the negligent behavior of the dialysis patients toward their oral health. Many patients receiving dialysis are victims of oral neglect. Dialysis is time consuming and often leaves individuals with lowered self-esteem. Strategies should be designed to facilitate provision of dental education within the premises of the institutes so that the individuals will be able to receive oral health care instruction regarding the possible complications of poor dental health.
Extensive literature reviews showed that very few studies were conducted to assess the periodontal status by using WHO basic oral health survey methodology 1997. This fact implies that the important, but so far understudied issue of prevalence and severity of periodontitis in CKD patients require standardized approach.
In this study, there was statistically significant difference between the dialysis and control group based on the highest CPI and LOA score. This is in accordance with the studies conducted by Davidovich et al.,[2] Naugle et al.,[8] Marakoglu et al.,[9] Murthy et al.,[17] and Marinho et al.[24] This might be due the fact that the patients receiving dialysis are preoccupied with their main life-threatening problem, neglect basic preventive oral care. Stress and frustration due to dietary restriction were found to contribute to anxiety reactions or depression. Efforts should be made to emphasize the importance of early intervention in dental health with follow-up care, including periodontal therapy and restorative treatment within 6 months of starting dialysis treatment.
Analysis of the effect of the duration of dialysis on the periodontal tissues of patients with CRF showed no difference among the subgroups, which is in accordance with the result of Naugle et al.,[8] Marakoglu et al.,[9] Bots et al.,[23] and Cengiz et al.[25] Although there was tendency for all clinical parameters (including oral hygiene status and the periodontal status) that were assessed in this study to get worsen significantly with increase in the duration of dialysis as reported by Davidovich et al.,[2] but these findings did not reach the significant level in this study. However, this tendency might indicate the presence of an inverse relationship between duration of chronic kidney disease, which is a chronic and deteriorating process, and quality of personal oral hygiene. This result supports the suggestion that although uremic state causes immune-suppressed state as a result of increased toxins, the host is still able to mount a partial response to bacterial challenge, due to the fact that these patients are not completely immune deficient.[9]
The limitations of this study include its performance in two renal institutes and relatively on small sample, but comparable with most of the previous studies, this may not be large enough to represent the CKD population. Also, our findings may be limited because only the physical measurement of periodontal disease was made and not the effect of biochemical markers (Serum calcium, serum phosphorus, serum hsCRP) on periodontitis was made. There may be important differences in the host response to bacterial challenges. Moreover, in this study partial mouth recordings protocol was used for the estimation of periodontal diseases that may be accurate and efficient in estimating the mean periodontal measures but could severely under and/or over-estimate the prevalence of periodontal disease.
In summary, the periodontal status was poor among the patients receiving hemodialysis as compared to the healthy control group. Therefore, within the limitation of the study, it can be concluded that periodontal disease is more common, prevalent, severe, and unrecognized in CRF patients. The results also suggested that higher prevalence of the periodontal diseases in CRF patients is mainly due to the negligence of the oral hygiene rather than of chronic uraemia in the CRF population. Prophylaxis and early dental care should be intensified in CRF patients; this may have a beneficial impact on their general health status. A larger series of patients and longitudinal studies are needed to confirm our findings and validate the hypothesis.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Renal disease. In: Lynch MA, Brightman VJ, Greenberg MS, eds. Burket's Oral Medicine (9th ed). Philadelphia: J.B. Lippincott Co; 1994. p. :487-509.
- [Google Scholar]
- Oral findings and periodontal status in children, adolescents and young adults suffering from renal failure. J Clin Periodontol. 2005;32:1076-82.
- [Google Scholar]
- Dental considerations for the patients with renal disease receiving hemodialysis. J Am Dent Assoc. 1996;127:211-9.
- [Google Scholar]
- Oral health in Brazilian patients with chronic renal disease. Rev Méd Chil. 2008;136:741-6.
- [Google Scholar]
- Interactions between chronic renal disease and periodontal disease. Oral Dis. 2008;14:1-7.
- [Google Scholar]
- The oral health status of individuals on renal dialysis. Ann Periodontol. 1998;3:197-05.
- [Google Scholar]
- Periodontal status of chronic renal failure patients receiving hemodialysis. Yonsei Med J. 2003;44:648-52.
- [Google Scholar]
- Oral health survey basic methods. In: World health organization (4th ed). Geneva. Delhi: AITBS Publisher and Distributors; 1997. p. :16-20.
- [Google Scholar]
- Statistical Package for Social Science (SPSS) version 17. Chicago, III: SPSS Inc; 2008.
- Oral hygiene profile of subjects on renal dialysis. Indian J Dent Res. 2001;12:71-6.
- [Google Scholar]
- Assessment of oral status of patients undergoing renal dialysis in a hospital at Bangalore city. J Indian Assoc Public Health Dent. 2005;5:35-8.
- [Google Scholar]
- The periodontal status of pre-dialysis chronic kidney disease and maintenance dialysis patients? Nephrol Dial Transplant. 2007;22:457-64.
- [Google Scholar]
- Oral and dental manifestations in diabetic and non diabetic uremic patients receiving hemodialysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99:689-95.
- [Google Scholar]
- Renal function and periodontal disease in elderly Japanese. J periodontol. 2007;78:1241-8.
- [Google Scholar]
- Dental diseases in Jordanian population on renal dialysis. Quintessence Int. 2003;34:343-7.
- [Google Scholar]
- The oral health status of dentate patients with chronic renal failure undergoing dialysis therapy. Oral Dis. 2006;12:176-80.
- [Google Scholar]
- Oral health status in patients with moderate-severe and terminal renal failure. Med Oral Patol Oral Cir Bucal. 2007;12:E305-10.
- [Google Scholar]
- The effect of the duration of the dialysis in hemodialysis patients on dental and periodontal findings. Oral Dis. 2009;15:336-41.
- [Google Scholar]




