

Translate this page into:
Refeeding Syndrome in Haemodialysis Patients
Address for correspondence: Dr. Prawash K. Chowdhary, Ramkrishna Care Hospital Raipur - 492 001, Chhattisgarh, India. E-mail: prawashchowdhary@yahoo.co.in
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Nutritional therapies have shown to be efficacious and efficient, despite the overall low level of evidence. It however hides the risk of refeeding syndrome in catabolic malnourished patients. Refeeding syndrome is the metabolic response due to the switch from a starvation to a fed state in the initial phase of nutritional therapy in patients who were severely malnourished or metabolically stressed due to severe illness. Here we describe two cases of chronic kidney disease patients on maintenance haemodialysis, who developed refeeding syndrome. Both the patients had tuberculosis and were severely malnourished with subjective global Assessment (SGA) of grade C. Timely diagnosis and proper management leads to good outcome.
Keywords
Haemodialysis
hypophosphatemia
refeeding

Introduction
Refeeding Syndrome is a serious and potentially fatal disorder in severely malnourished patients, supported enterally or parenterally. It is caused by an intracellular shift of fluids, sodium, potassium, magnesium and phosphorus as well as changes in the metabolism of glucose, protein, fats and vitamins resulting from the enhanced insulin secretion in response to caloric load.[1] Metabolic changes include hypophosphatemia, hypokalemia, hypomagnesemia, sodium retention and hyperglycemia.[2] If severe, refeeding syndrome may result in respiratory, cardiac and neuromuscular dysfunction. Although hypophosphatemia is a hallmark of refeeding syndrome, renal dysfunction might hide refeeding hypophosphatemia, especially in maintenance haemodialysis patients (MHD).[3]
Uremic malnutrition, also referred to as protein-energy wasting (PEW), represents a disorder with increasing incidence in preterminal as well as end-stage renal disease (ESRD) patients. Prevalence of PEW is reported to vary between 10% and 36% in these patients.[4] Affected patients will experience high morbidity, leading to reduced survival. National guidelines strongly support nutritional intervention in all MHD patients.[5] Several attempts have been undertaken to combat the PEW in MHD patients, either with oral supplements or with intradialytic parenteral nutrition (IDPN). IDPN is a therapeutic approach to treating malnourished patients on MHD.[6]
Case Report
Case 1
A 64-year-old man renal allograft recipient (year of Transplant -2012), known case of Type 2 Diabetes Mellitus, Hypertension, Coronary artery disease with moderate Left ventricular dysfunction had, chronic graft dysfunction leading to ESRD. He was on regular MHD, thrice weekly from Feb 2019. He was chronic alcoholic. He presented with, complaints of generalised weakness and decreased appetite for 3 months and low grade fever without chills for 1 month. He had lost 8 kg weight in 6 months. On examination he was conscious and well oriented. He was febrile with pulse of 90/min, Blood pressure of 150/70 mm Hg and respiratory rate of 18/min. His body weight was 55 kg with body mass index of 18.6 kg/m2 and has subjective global assessment of grade C suggestive of severe malnutrition.
His blood parameter were: Haemoglobin (6.6 gm/dl), WBCs count (6180 cmm/mm), Platelet count (1.6 lakhs/cmm), Serum sodium (142 meq/L) serum potassium (4.6 meq/L), serum Magnesium (2.4 mg/dl), Serum calcium (8.8 mg/dl), serum phosphorus (5.8 mg/dl), Serum creatinine (6.8 mg/dl) with normal liver functions except low serum albumin (2.1 mg/dl). His Chest X ray PA view was normal, Ultrasonography showed bilateral small size kidney, fundus examination showed evidence of bilateral proliferative diabetic retinopathy, Electrocardiogram (Sinus Tachycardia), echocardiogram showed low ejection fraction (45%). His upper gastrointestinal endoscopy showed oesophageal candidiasis.
Patient was managed with Antibiotics (Amoxycillin-Clavulanate), and Antifungal (Fluconazole) drugs, blood transfusion and regular MHD. As he was anorexic, Ryle's tube feeding was started, 1800 K calories with 55 gm protein by continuous feed (40 ml/hr) consisting of total volume of 960 ml in 24 hours. On 3rd day he developed altered sensorium with bilateral pitting oedema. His heart rate was 132/min irregularly irregular with respiratory rate of 28/min and blood pressure of 90/60 mm Hg. His ECG was suggestive of Atrial Fibrillation shown in Figure 1. Cardiology consultation was taken. He was intubated and put on ventilatory support. Repeat Chest Xray was suggestive of bilateral pleural effusion. Repeat serum electrolyte showed serum sodium (122 meq/L), serum potassium (2.8 meq/L), serum magnesium (1.5 mg/dl), serum calcium (8.2 mg/dl) and serum phosphorus (1.6 mg/dl). Enteric nutrition was interrupted. Dyselectrolaemias (Serum phosphorus, magnesium and potassium) were corrected. Initially phosphorus and potassium replacement were done with 45 mmol potassium phosphate intravenously over 8-12 hrs, levels were checked and repeat infusion was given if necessary. Later on, replacement was done with oral supplementation of Sodium Acid Phosphate sachet and syrup potassium chloride as per requirement. IV magnesium replacement with 20-24 mmol MgSO4 (4-6 g) over 6-8 hrs was done and the level was reassessed every 8-12 hours. He also received once daily dose of Thiamine (initially 200 mg then 100 mg) and Vitamin B12 (1 mg). In addition, a hydrocortisone injection 100 mg was given to prevent adrenal insufficiency. Initially intravenous replacement of phosphorus was done followed by oral replacement. Once daily dose of Vitamin B12, Thiamine and Hydrocortisone were also given, Trace elements were supplemented. Antibiotics were upgraded to Piperacillin-Tazobactum. Patients was detected to have disseminated Tuberculosis, antituberculosis drug were started as per dose modification. Gradually his general condition improved, ventilatory support was withdrawn. On the 8th days when his blood chemistry became normalised, enteric nutrition were resumed at 500 kcal/day, which was gradually increased. He was discharged on day 15 with normal serum electrolytes. Details of patient electrolyte changes during hospital stay is shown in Table 1.

- ECG of case1 showing Atrial fibrillation
| Timeline | At Admission | 3rd day | 6th day | 8th day | 10th day | 12th day | 15th day Discharge, day |
|---|---|---|---|---|---|---|---|
| Serum Sodium Meq/L | 142 | 122 | 131 | 138 | 140 | 139 | 142 |
| Serum Potassium, meq/L | 4.6 | 2.8 | 3.3 | 4.2 | 4.1 | 4.4 | 4.2 |
| Serum Magnesium, mg/dl | 2.4 | 1.5 | 1.8 | 2.1 | 2.2 | 2.1 | 2.4 |
| Serum Calcium Mg/dl | 8.8 | 8.2 | 8 | 8.6 | 8.4 | 8.2 | 8.6 |
| Serum Phosphorus, mg/dl | 5.8 | 1.6 | 2 | 2.8 | 3.2 | 3.4 | 3.8 |
Case 2
A 53-year-old female, case of neurogenic bladder, ESRD and was on MHD twice a weekly for 2 year. She had abdominal tuberculosis and was on antitubercular drugs for 2 months. She had generalised weakness and decreased Appetite for 3 months. She had lost 6 kg weight in 3 months. On examination she was conscious and well oriented, with pulse of 78/min, Blood pressure of 160/80 mm Hg and respiratory rate of 16/Min. Her body weight was 46 kg, Body Mass Index of 16.8 kg/m2 with subjective global assessment of grade C suggestive of severe malnutrition. She was cachexic and had decreased appetite. Patient was advised thrice week haemodialysis with intradialytic parenteral nutrition. On Monday during haemodialysis she received IV Amino Acids (7%, 500 ml volume). On Tuesday her serum potassium, magnesium and phosphorus were 4.9 meq/L, 2.4 mg/dl and 5.6 mg/dl respectively. Dialysis fluid potassium level was 2 meq/L. On Wednesday during haemodialysis, intradialytic parenteral nutrition was started (1026 ml volume, total calories 900 kcal, Glucose 100 gm, Amino acids 34 g, Intralipid 40 g) at a rate of 200 ml/hr through venous line. After 3 ½ of dialysis, she developed hypotension. Cardiac monitor showed sustained ventricular tachycardia (VT). ECG of patients is shown in Figure 2. Emergency blood gas analysis was done which showed hypokalaemia (Serum potassium 2.6 meq/L). Cardiopulmonary resuscitation was done, 3 cycles of DC shock were given. After rhythm got normalised, 12 leads ECG done showed QTc prolongation, shown in Figure 2. Patients was admitted. Cardiology consultation taken. There was no evidence of acute coronary syndrome. Serum electrolyte were done. Her serum potassium, magnesium and phosphorus were 2.8 meq/L, 1.4 mg/dl and 1.9 mg/dl, respectively. Dyselectrolaemia were corrected. She received intravenous Thiamine and vitamin B12. Once clinical condition improved and serum electrolyte were corrected, enteral feeding was started through Ryle's Tube with 500 kcal, which was gradually increased. She was discharged on 10th day.
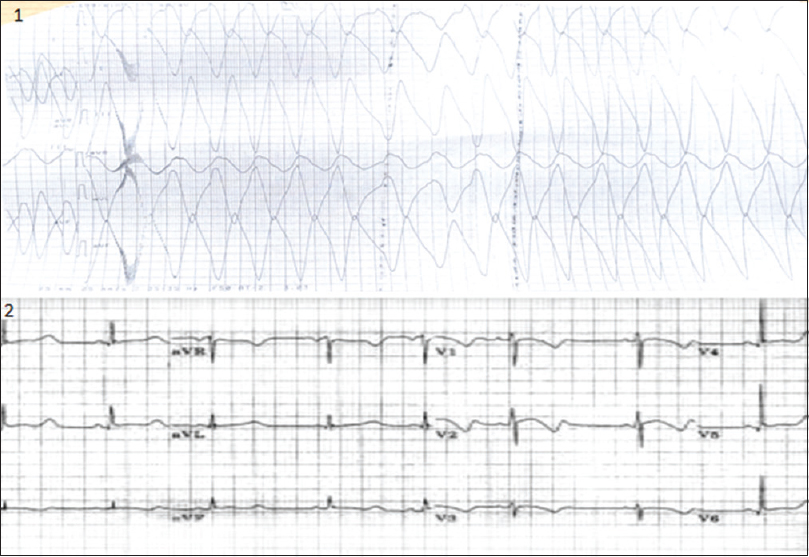
- ECG of case 2, 1. showing Ventricular tachycardia and 2. showing prolonged QTc interval
Discussion
Refeeding syndrome is a complication of acute nutritional rehabilitation (oral, enteral or parenteral) in individuals who are undernourished. In starvation, the body shifts from an anabolic metabolism to a state of catabolism in an effort to compensate for lack of available energy. These changes results in a shift from carbohydrate metabolism to protein and fat catabolism. The metabolism of proteins results in a breakdown of lean body mass, which directly affects major organs. In the heart, atrophy of the myocardium causes poor contractility and decreased cardiac output. Atrophy of liver causes decreased protein production, which exacerbates the metabolic state. Additionally, during starvation there is intracellular loss of electrolytes (potassium, magnesium and phosphate). Insulin secretion decrease, the basal metabolic rate slows down and the body becomes hypothermic and hypotensive, all in an effort to conserve protein and organ function.[7]
When nutritional rehabilitation is started, the body immediately shifts to an anabolic state, metabolising carbohydrates instead of proteins and fat. This new glucose load causes the body to increase insulin secretion and cell begins to uptake glucose, potassium, magnesium and phosphate.[7] This leads to hypokalemia, hypomagnesemia and hypophosphatemia. Additionally, insulin has an antinatriuretic effect on the kidneys, resulting in sodium retention and an increase in extracellular volume.[7]
There is no standardised definition of Refeeding Syndrome, however, there are proposed clinical criteria by the National Institute for Health and Clinical Excellence for identifying patients at high risk for refeeding syndrome. Table 2 outlines a risk stratification tool for adults (8). The National Institute for Clinical Excellence[8] and British Association of Parenteral and Enteral Nutrition guidelines[9] has proposed the guidelines for management, which is shown in Figure 3.
| One of the following: |
| Body mass index (BMI)<16 kg/m2 |
| Unintentional body weight loss>15% in the preceding 3 to 6 months |
| Very little or no nutritional intake for>10 days |
| Low concentrations of plasma potassium, phosphate or magnesium prior to feed |
| Or two of the following: |
| BMI<18.5 kg/m2 |
| Unintentional body weight loss>10% in the preceding 3 to 6 months |
| Very little or no nutritional intake for>10 days |
| History of alcohol or drug abuse |
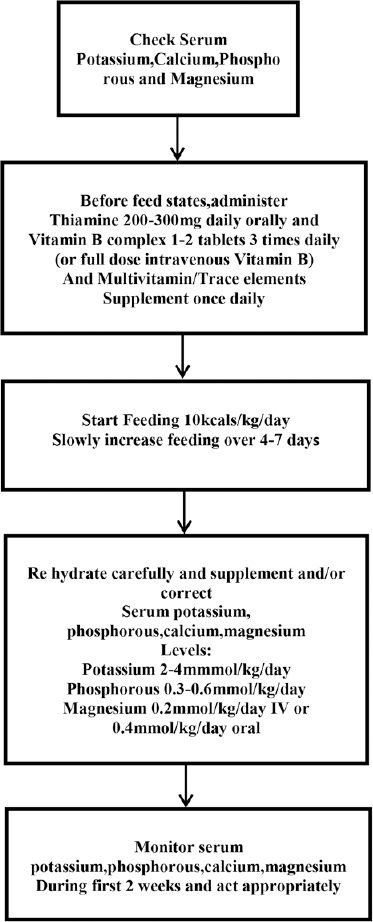
- Guidelines for Re feeding Syndrome Management. Adapted for NICE(8) and British Association of Parenteral and enteral Nutrition guidelines(9)
In the first case, according to NICE guidelines, patient has three risk factors for Refeeding syndrome: BMI of 18.6 kg/m2, weight loss >10% (weight decrease from 63 kg to 55 kg) in 3-6 month and he was chronic alcoholic. As per guidelines total calories intake for this patient should have been 10 kcal/kg/day i.e., 550 kcal per day. But our patients received calories intake of 1800 kcal/day; 32.7 kcal/kg/day. So, he developed refeeding syndrome. With early diagnosis and proper treatment patient recovered and discharged from hospital.
Intradialytic parenteral nutrition is a method of parenteral nutrition through the venous drip chamber of the haemodialysis circuit while the patients is receiving haemodialysis.[10] Various guidelines are being proposed by British Columbia Renal Agency[10] and European Renal Association-European Dialysis and Transplant Association[11] to define the indications for IDPN. Our patients had abdominal tuberculosis with poor appetite. She was severely malnourished, had SGA of grade C. She had a weight loss of >10% in 3-6 months with low serum albumin (2.6 mg/dl). Hence intradialytic parenteral nutrition was started.
In the second case, according to NICE guidelines, patient had two risk factors for RFS: BMI of 16.8 kg/m2 and weight loss >10% (weight loss from 52 kg to 46 kg) in 3-6 month. As per guidelines total calories intake should have been 10 kcal/kg/day. So the appropriate administration rate of IDPN should have been be 19.1 kcal/h (10 kcal × 46 kg = 460 kcal/day: 460 kcal/24hr = 19.1 kcal/hr). But patient received IDPN at a rate of 180 kcal/hr (900 kcal/5 hr = 180 kcal/hr), which was 10 times higher than the recommended amount.
Patient serum potassium, magnesium and phosphorus one day before haemodialysis were 4.9 meq/L, 2.4 md/dl and 5.6 mg/dl, respectively. Post haemodialysis her serum potassium, magnesium and phosphorus were 2.8 meq/L, 1.4 mg/dl and 1.9 mg/dl respectively. This rapid decrease in serum electrolytes besides removal by haemodialysis is also due to intracellular shift of electrolyte, suggestive of refeeding syndrome. We cannot completely exclude the possibility of idiopathic VT unrelated to IDPN and HD. However, because continuous ECG monitoring did not detect VT recurrence after supplementation of essential elements, it is reasonable to consider that the VT was triggered by electrolyte abnormalities such as hypokalemia and hypomagnesemia exacerbated by IDPN and haemodialysis.
Based on the risk stratification of refeeding syndrome, total parenteral nutrition with a slow rate of calorie infusion, instead of IDPN, should be preferred, especially for patients ending a considerable period of fasting. If IDPN must be selected for such patients, its starting dose should be reduced.
Conclusion
Refeeding syndrome is a highly challenging metabolic situation, leading to potentially life-threatening complications with fluid and electrolyte disturbances. Refeeding syndrome should therefore be timely and adequately treated. When IDPN for malnourished haemodialysis patients is considered, the risk of refeeding syndrome should be fully assessed and managed before starting IDPN.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Refeeding and metabolic syndrome: Two sides of the same coin. Nutr Diabetes. 2014;4:e120.
- [Google Scholar]
- Nutrition and renal disease. In: Greenberg A, ed. Primer on Kidney Disease. Academic Press; 1998. p. :440-7.
- [Google Scholar]
- ESPEN guidelines on parenteral nutrition: Adult renal failure. Clin Nutr. 2009;28:401-14.
- [Google Scholar]
- Malnutrition in haemodialysis patients: What therapy? Am J Kidney Dis. 2005;46:371-86.
- [Google Scholar]
- National Institute for Health and Clinical Excellence. Nutrition support in adults Clinical guideline CG32 2006
- [Google Scholar]
- Refeeding syndrome. In: Todorovic VE, Micklewright A, eds. A Pocket Guide to Clinical Nutrition (2nd ed). British Dietetic Association; 2011.
- [Google Scholar]
- BC Renal Agency: Intradialytic Parenteral Nutrition (IDPN) Available from: http://WWW.bcrenalagency.ca/resource-gallery/ Documents/IntradialyticParenteralNutrition (IDPN).pdf
- [Google Scholar]




