

Translate this page into:
A Prospective Comparison of Outcomes of Brachiocephalic Versus Brachiobasilic Fistulas for Hemodialysis
Corresponding author: Joel Mathew John, Department of Vascular Surgery, Christian Medical College Vellore, Vellore, Tamil Nadu, India. E-mail: jmj8587@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: John JM, Mithra LSP, Reddy YG, Selvaraj AD, Premkumar P, Samuel V. A Prospective Comparison of Outcomes of Brachiocephalic Versus Brachiobasilic Fistulas for Hemodialysis. Indian J Nephrol. 2025;35:40-5. doi: 10.25259/ijn_367_23
Abstract
Background
Brachiocephalic fistula (BCF) and brachiobasilic fistula (BBF) are autogenous fistulas created in the arm for hemodialysis access. However, despite the differences in anatomy and surgical technique, the existing literature shows no significant statistical difference between the maturation, patency, or complications. We analyzed the outcomes of these two types of arteriovenous fistulas in our subgroup of the Indian population.
Materials and Methods
A prospective observational cohort study was performed at a tertiary hospital from August 2019 to August 2021 between patients who underwent BCF and BBF. The time to maturation, 1-year primary patency, and postoperative complications were studied.
Results
Among the 236 patients, 137 and 99 underwent BCF and BBF, respectively. 53 (39%) and 37 (37.4%) patients were lost to follow-up at the end of 12 months in each arm, respectively. Each group comprised predominantly of males. There was no significant difference in age, diabetes, coronary artery disease, or peripheral arterial disease between the groups. The time to maturation within 6 weeks, more than 6 weeks, and non-maturation was 51.88% and 58.1% (p = 0.58), 38.67% and 32.55% (p = 0.04), and 9.43% and 9.3% (p = 0.74) in BCF and BBF groups, respectively. The 1-year primary patency, primary-assisted patency, and secondary patency were 69.04% and 53.22% (p <0.001), 78.3% and 59.6%, and 79.5% and 62.9% in BCF and BBF groups, respectively. Apart from venous hypertension (BCF:2(1.5%) vs BBF:7(7.1%), p = 0.026), there were no significant differences in the postoperative complications between the groups.
Conclusion
BCFs take longer to mature but have greater primary patency than BBF. Both of these fistulas had similar postoperative complications. Larger randomized trials are needed to confirm our findings.
Keywords
Arteriovenous fistula
Brachiocephalic
Brachiobasilic
Chronic kidney disease
Hemodialysis access

Introduction
The National Kidney Foundation Dialysis Outcomes Quality Initiative (KDOQI) has guidelines regarding the order of preference for the creation of arteriovenous fistulas (AVFs) for hemodialysis access. Brachiocephalic fistula (BCF) and brachiobasilic fistula (BBF) are autogenous fistulas that can be created in the arm. However, there is conflicting data regarding the usability, safety, and patency of BBFs with respect to BCFs.1-5 The limited data from randomized studies prevent its widespread application compared to that of BCFs.2
There are multiple anatomical advantages of choosing the basilic vein over the cephalic vein for creating AV fistulas.2 The basilic vein is naturally deeper, less prone to damage from previous venepunctures, and larger in caliber.3 However, these advantages demand more complex surgical techniques and prolonged surgery. Hence, the procedure is usually performed under regional anesthesia or general anesthesia.6
On the other hand, the cephalic vein is more superficial, easily damaged by previous venepunctures, and requires a simpler surgical technique. However, there is no consensus on which type of AVF is preferred when their respective outcomes are directly compared.2,3,7,8
The KDOQI guidelines recommend the preference for AVF placement to be a radiocephalic AVF followed by a brachiocephalic AVF and if any of these are not viable, then a brachiobasilic AVF should be created.4 However, no evidence based on prospective randomized trials supports this recommendation.9
There were also certain patient characteristics and factors that were reported to be associated with poorer outcomes in patients with upper arm AVFs: older age, female sex, obesity, previous vascular access, peripheral vascular disease, and ipsilateral central venous catheterization.1,10-12
The overall patency of AVFs in the Indian population has been lower. The 3-year primary and secondary patencies of the RCF, BCF, and BBF groups were 43.6%, 58.6%, 42.6% and 47.3%, 62.5%, 56.9%, respectively.13,14
We aimed to analyze the outcomes of autogenous AVFs created in the arm for hemodialysis access in patients diagnosed with chronic kidney disease. Specifically, we measured the time to maturation, primary patency, and complications following the creation of a BCF versus a BBF.
Materials and Methods
This prospective observational cohort study was carried out after scientific and ethical approval from the Institutional Review Board (IRB), Christian Medical College Vellore, India (IRB Min. No. 12290, dated 08.10.2019) from August 2019 to August 2021.
All the study participants were evaluated and recruited into study groups in the outpatient department and inpatient wards of the Department of Vascular Surgery in a tertiary hospital in south India from August 2019 to August 2021.
All study subjects were above 18 years of age, diagnosed with chronic kidney disease stage 5, and were undergoing hemodialysis or required a preemptive hemodialysis arteriovenous access. The medical history and physical examination, including ultrasound duplex screening, were performed by a member of the surgical team. Participants who had previously undergone a radiocephalic fistula or any arterial surgical procedure involving the hand or forearm were excluded. After providing informed consent, an ultrasound duplex screening of the upper limb was performed at room temperature and the venous diameter was measured after applying a tourniquet to the upper arm. On an ultrasound duplex, the diameter of the brachial artery should be ≥3 mm. Patients who underwent BBF with or without adjunctive superficialization or transposition procedures were also included.
We excluded patients who were unable to provide informed consent or who had a non-palpable radial or ulnar pulse. We also excluded patients with any clinical or venographic features of proximal vein obstruction.
As per the algorithm shown in Figures 1 and 2, patients underwent clinical examination and an ultrasound duplex scan. Those without palpable radial or ulnar pulses in the upper limb were excluded from further evaluation. Patients who were suitable for a forearm AVF on subsequent ultrasound duplex evaluation were also excluded. The size of the brachial artery was then measured, and only patients with a diameter ≥3 mm underwent further evaluation; others were excluded. The diameter of the cephalic vein at the level of the elbow or distal forearm was then measured, and those with a vein ≥2.5 mm were recruited into the BCF arm. If the cephalic vein diameter was smaller, assessment of the basilic vein diameter followed; patients whose basilic vein diameter was ≥2.5 mm were recruited into the BBF arm.
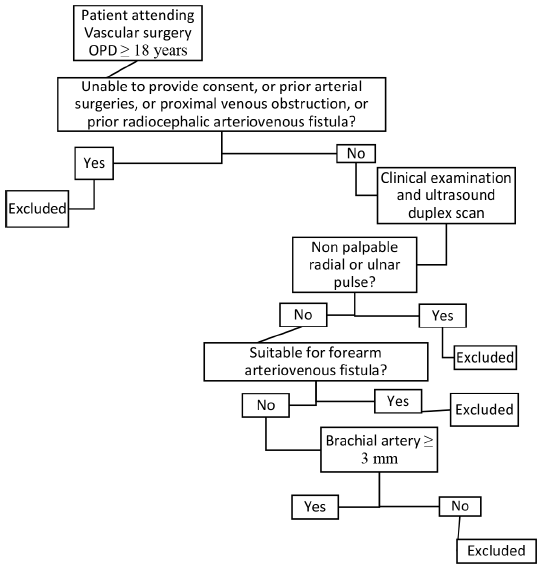
- Patient allocation algorithm – Part 1. OPD: Outpatient department.
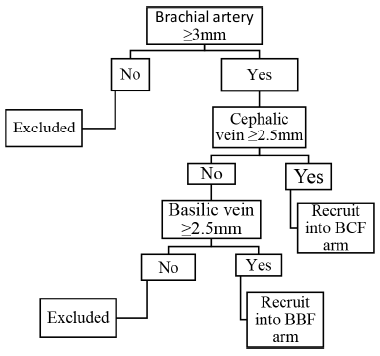
- Patient allocation algorithm – Part 2. BCF: Brachiocephalic fistula; BBF: Brachiobasilic fistula.
The surgical procedure was performed independently or under the direct supervision of a consultant vascular surgeon with at least 3 years of experience in fistula creation and salvage procedures. Participants recruited into the BCF group predominantly underwent the surgery under local anesthesia. Participants in the BBF group underwent the procedure under brachial plexus block if a superficialization/transposition procedure was performed or at a later stage.
Patients were discharged on the second postoperative day. Each group was then advised to undergo follow-up assessments at the outpatient department within 1 week, at 4 weeks, and again at 6 weeks, with subsequent visits every 2 weeks until successful maturation or cannulation. All participants were required to have a follow-up period of at least 12 months and during these visits, they underwent clinical examinations as well as ultrasound duplex examinations.
Outcomes and variables
The following outcomes were measured in each group:
Maturation – Ability to perform two-needle cannulation for adequate hemodialysis for at least a continuous period of 4 weeks. The presence of continuous thrill and duplex ultrasound findings with flow volume >600 mL/min; vein diameter >6 mm; and vein depth <6 mm aided in the diagnosis of maturation of the fistula.
Time to maturation: The period until the primary fistula was suitable for successful cannulation for hemodialysis. This was classified into ≤6 weeks, >6 weeks, or non-maturation.
Non-maturation: Inability to perform two-needle cannulation for adequate hemodialysis by 12 months after the surgical procedure.
Primary patency – The time interval from fully functional access placement until any intervention designed to maintain or re-establish patency, access thrombosis, or the time of measurement of patency.
Primary-assisted patency: The time interval from access placement to access thrombosis when intervening manipulations (surgical or endovascular) were performed to maintain the functionality of the patent’s access.
Secondary patency: Time interval from the time of fully functional access placement until access abandonment, thrombosis, or the time of patency measurement including intervening manipulations designed to re-establish functionality in thrombosed access.
Patients who failed to maintain follow-up at the outpatient clinic or inpatient department were excluded from analysis of patency rates.
Postoperative/surgical complications
Seroma, hematoma, surgical site infection, pseudoaneurysm, steal syndrome, venous hypertension, immediate thrombosis (less than 30 days), and mortality (within a year) were recorded in the postoperative period.
According to Koksoy et al.,9 the primary patency of BCF and BBF at 3 years was 81% and 73%, respectively. Assuming a primary patency of 80% in BCF and 65% in BBF, with 80% power and 5% alpha error, the sample size of the study population was estimated to be 138 in each group.
Summary data are presented as the mean ± SD for normally distributed data and as the median with interquartile range (IQR) if data were skewed. The categorical variables are presented as numbers and percentages. The characteristics of BCF and BBF were compared using t-test and categorical data were compared using Chi-square/Fisher’s exact test as appropriate. Statistical significance was defined as p ˂ 0.05. All analyses were performed using SPSS version 25.
Results
As indicated in Figure 3, 236 patients with chronic kidney disease requiring arteriovenous access were recruited for the study from August 2019 to August 2021. According to the above inclusion criteria, 137 and 99 patients underwent BCF and BBF creation procedures, respectively. As the study took place during the COVID-19 pandemic, the intended sample size could not be reached due to lockdowns and restrictions.
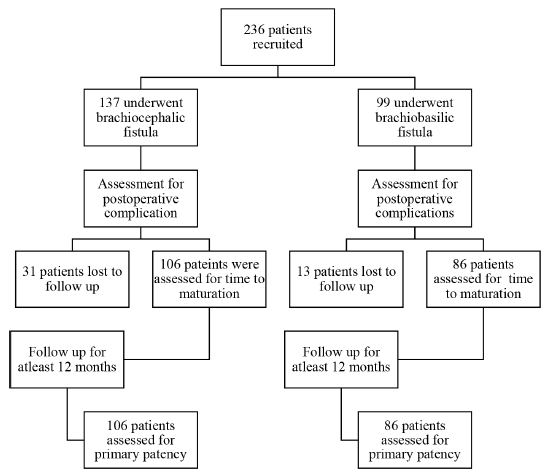
- Methodology.
The demographic characteristics and distribution of the study population in each group are listed in Table 1.
| Patient characteristic | BCF (n = 137) | BBF (n = 99) | p value |
|---|---|---|---|
| Male: Female | 1.36:1 | 1.6:1 | 0.54 |
| Age | 48.26 ± 13.49 | 51.29 ± 14.46 | 0.47 |
| Diabetes | 63 (46%) | 48 (48.5%) | 0.7 |
| Coronary artery disease | 24 (17.5%) | 22 (22.2%) | 0.36 |
| Peripheral arterial occlusive disease | 8 (5.8%) | 3 (3%) | 0.31 |
| Brachial artery size (mm) | 3.93 ± 0.69 | 3.93 ± 0.64 | 0.175 |
| Vein size (mm) | 3.66 ± 0.79 | 3.71 ± 0.85 | 0.569 |
BCF: Brachiocephalic fistula; BBF: Brachiobasilic fistula.
Both the study groups were comprised predominantly of males, and there was no significant statistical difference between the groups. The mean ages of the individuals in the BCF and BBF groups were 48.26 ± 13.49 years and 51.29 ± 14.46 years, respectively. There was no significant statistical difference between the study groups with respect to pre-existing medical comorbidities such as diabetes mellitus, coronary artery disease, or peripheral arterial occlusive disease. In the BCF group, the mean sizes of the brachial artery and cephalic vein were 3.93 ± 0.69 mm and 3.67 ± 0.79 mm, respectively. In the BBF group, the mean sizes of the brachial artery and basilic vein were 3.93 ± 0.64mm and 3.71 ± 0.85mm, respectively.
In the BBF group, 16 (16.2%) patients did not require superficialization/transposition, 35 (35.4%) underwent superficialization, and 48 (48.4%) underwent transposition.
Time to maturation
The impact of the COVID-19 lockdown and travel restrictions was also reflected in our measurement of the primary outcomes, as listed in Table 2. After the primary surgical procedure, 22.6% and 13.1% of the patients in the BCF and BBF groups, respectively, were lost to follow-up. In the BCF group, the time to maturation/successful cannulation was 51.8% and 38.6% within 6 weeks and after 6 weeks, respectively. In the BBF group, the time to maturation/successful cannulation was 58.1% and 32.5% within 6 weeks and after 6 weeks, respectively. The greater proportion of BCF patients who matured beyond 6 weeks was found to be statistically significant (p value 0.04). A total of 9.43% and 9.3% of the BCF and BBF groups, respectively, failed to mature and could not be successfully cannulated for hemodialysis.
| Outcome | BCF (n = 106) | BBF (n = 86) | p value |
|---|---|---|---|
| Time to maturation | |||
| ≤6 weeks | 55 (51.88%) | 50 (58.1%) | 0.58 |
| >6 weeks | 41 (38.67%) | 28 (32.55%) | 0.04 |
| Nonmaturation | 10 (9.43%) | 8 (9.3%) | 0.74 |
| Primary patency | |||
| 12 months | 58 (69.04%) | 33 (53.22%) | 0.001 |
| Primary access failure | |||
| ≤3 months | 13 (15.47%) | 19 (30.64) | 0.21 |
| 3–6 months | 6 (7.14%) | 4 (6.45%) | 0.65 |
| 6–12 months | 7 (8.33%) | 6 (9.67%) | 1.01 |
BCF: Brachiocephalic fistula; BBF: Brachiobasilic fistula.
Patency rates
To measure the outcome of primary patency, all study group participants were advised to follow up for at least 12 months. However, 39% and 37.4% of the BCF and BBF group subjects, respectively, were lost to follow-up at the end of 12 months and hence were excluded from analysis of primary patency rates.
The primary patency and access failure rates of the BCF and BBF patients at different time intervals are also listed in Table 2. The primary patency of BCF and BBF subjects at 12 months were 69.04% and 53.22%, respectively. The higher 12-month primary patency of BCF was statistically significant (p value 0.001).
The primary-assisted patency rates for BCF and BBF at 12 months were 78.3% and 59.6%, respectively. The secondary patency rates for BCF and BBF at 12 months were 79.5% and 62.9%, respectively.
Complications
The postoperative surgical complications in each group are listed in Table 3. There was no statistically significant difference among the majority of the various complications between the study groups. However, we found that the incidence of postoperative central venous hypertension was significantly greater in the BBF group (p value 0.026).
| Complications | BCF (n = 137) | BBF (n = 99) | p value |
|---|---|---|---|
| Seroma | 3 (2.2%) | 0 (0%) | 0.138 |
| Hematoma | 1 (0.7%) | 1 (1%) | 0.817 |
| Surgical site infection | 1 (0.7%) | 0 (0%) | 0.394 |
| Pseudoaneurysm | 1 (0.7%) | 3 (3%) | 0.177 |
| Steal syndrome | 1 (0.7%) | 0 (0%) | 0.394 |
| Venous hypertension | 2 (1.5%) | 7 (7.1%) | 0.026 |
| Immediate thrombosis (≤30 days) | 3 (2.2%) | 5 (5.1%) | 0.231 |
| Mortality (within 1 year) | 7 (5.1%) | 6 (6.1%) | 0.752 |
BCF: Brachiocephalic fistula; BBF: Brachiobasilic fistula.
We also performed a multivariate analysis using ANOVA test to assess whether the brachial artery size or the vein size had any effect on the time to maturation or primary access failure between the two groups, respectively. The p-values, as listed in Table 4, show that there was no significant statistical difference.
| ANOVA p value | ||
|---|---|---|
| Ultrasound duplex measurement | Time to maturation | Primary access failure |
| Mean brachial artery size | 0.993 | 0.47 |
| Mean vein size | 0.771 | 0.406 |
Discussion
Our data regarding the outcomes of AVFs created for hemodialysis are “real world” and strongly reflect the many practical and technical challenges in managing this relatively morbid subset of the population. This study was performed in a tertiary center with the multidisciplinary specialty teams available to facilitate adequate referral of patients in need of access to the vascular surgical team. As there were specific clinical and ultrasound duplex criteria before creating a BCF or a BBF, there was no significant difference in the demographic and medical characteristics between the two groups. It is no surprise that the majority of AVFs mature within 6 weeks, and this is also reflected in our cohort. The greater incidence of delayed maturation or nonmaturation of the BCF confirms the fact that the cephalic vein, due to its superficial location and a common venepuncture site, is more prone to be phlebitic.
The success of any community health program depends on its ability to spread awareness and educate the common man and affected population regarding the disease in question. It also includes education regarding the need for follow-up, detecting early signs of complications and the “when, how, and where” to seek help. We realized this vacuum in our healthcare practice when we reported a significant loss to follow-up in our cohort of patients. This was also aggravated by the ongoing COVID-19 lockdowns and restrictions that were in place. Overall, our patency rates are comparable to those in other available literature in the Indian population.13,14
One prospective study revealed no significant difference in the patency rates between the two types of AVF. Primary patency at 1 and 3 years of follow-up was 87% and 81%, respectively, for the BCF group and 86% and 73%, respectively, for the BBF group. The secondary patency rates at the 1- and 3-year follow-ups were 87% and 70%, respectively, for the BCF group; and 88% and 71% for the BBF group.9
Woo et al. reported that autogenous BBF and transposed BCF have similar patency rates. They reported that the primary and secondary patency rates were 52% and 62%, respectively, at 5 years for BBF and 40% and 46%, respectively, at 5 years for BCF.3 However, Ascher et al. reported higher 1-year patency rates for BCF and BBF, at 72% and 70%, respectively.5
BBF and BCF AVFs had similar maturation rates. Maturation rates were somewhat greater with BBF (96%) than with BCF (90%), but this difference did not reach statistical significance.9
The 1-year primary patency rates were significantly greater in our BCF group. This could be because the BCF surgical procedure is technically simpler and, as a consequence, a more familiar procedure for the operating team. Gibson et al. also found that simple AVFs had a superior patency compared to transposed fistulas.12
However, this had no significant impact on the immediate postoperative period in either group. There was no significant difference in the postoperative surgical complications or technical failure resulting in immediate access failure.
We also found that neither the brachial artery size nor the vein size significantly affected the primary outcomes as long as the baseline standard protocols were adhered to.
This study revealed the importance of patient selection, adequate postoperative follow-up, and the need for adequate facilities to educate patients regarding care and warning signs for impending access failure. In our rural and semi-urban community, we feel that the placement of more accessible surgical facilities and even specialized nursing staff can improve the outcomes of all our AVFs, thereby decreasing the morbidity in this vulnerable subset of the population.
The loss to follow-up, high dropout rate, impact of COVID-19, and lack of randomization may reduce the power of our statistical analysis. There was also a selection bias. Upon clinical and duplex assessment, if any patient was found suitable for both BCF and BBF fistulas, as per KDOQI guidelines, the preference was toward creating a BCF.
We need to analyze a larger randomized Indian population with more stringent selection and follow-up criteria before we can generalize our study findings.
We analyzed the outcomes of creating BCF and BBF fistulas in the Indian population and found that BCF may take longer to mature, but have a higher primary patency than BBF fistulas. Both of these autogenous AVFs had similar postoperative complications. More randomized trials, with larger sample sizes, are needed to confirm our findings.
Conflicts of interest
There are no conflicts of interest.
References
- Outcomes of upper arm rteriovenous fistulas for maintenance hemodialysis access. Arch Surg. 2004;139:201-8.
- [CrossRef] [PubMed] [Google Scholar]
- The brachial artery-basilic vein arteriovenous fistula in vascular access for haemodialysis-a review paper. Eur J Vasc Endovasc Surg. 2006;31:70-9.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the efficacy of the transposed upper arm arteriovenous fistula: A single institutional review of 190 basilic and cephalic vein transposition procedures. J Vasc Surg. 2007;46:94-101.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical practice guidelines for vascular access. Am J Kidney Dis. 2006;48:S176-S247.
- [CrossRef] [PubMed] [Google Scholar]
- The value and limitations of the arm cephalic and basilic vein for arteriovenous access. Ann Vasc Surg. 2001;15:89-97.
- [CrossRef] [PubMed] [Google Scholar]
- Superior maturation and patency of primary brachiocephalic and transposed basilica vein arteriovenous fistulae in patients with diabetes. J Vasc Surg. 1998;27:154-7.
- [CrossRef] [PubMed] [Google Scholar]
- Outcome after autogenous brachial-basilic upper arm transpositions in the post-national kidney foundation dialysis outcomes quality initiative era. J Vasc Surg. 2005;42:951-6.
- [CrossRef] [PubMed] [Google Scholar]
- Brachiobasilic arteriovenous fistula: different surgical techniques and their effects on fistula patency and dialysis-related complications. J Vasc Surg. 2003;37:821-6.
- [CrossRef] [PubMed] [Google Scholar]
- Brachiobasilic versus brachiocephalic arteriovenous fistula: A prospective randomized study. J Vasc Surg. 2009;49:171-7.
- [CrossRef] [PubMed] [Google Scholar]
- Basilic vein transposition fistula: a good option for maintaining hemodialysis access site options? J Vasc Surg. 2004;39:1043-7.
- [CrossRef] [PubMed] [Google Scholar]
- Vascular access outcomes using the transposed basilic vein arteriovenous fistula. Am J Kidney Dis. 2003;42:151-7.
- [CrossRef] [PubMed] [Google Scholar]
- Vascular access survival and incidence of revisions: A comparison of prosthetic grafts, simple autogenous fistulas, and venous transposition fistulas from the United States renal data system dialysis morbidity and mortality study. J Vasc Surg. 2001;34:69.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes of primary arteriovenous fistula for hemodialysis in elderly patients (>65 Years) with end stage renal disease: A study on indian population. Indian J Nephrol. 2019;29:387-92.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes and predictors of failure of arteriovenous fistulae for hemodialysis. Int Urol Nephrol. 2022;54:185-92.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




