

Translate this page into:
Cystatin C: An alternative dialysis adequacy marker in high flux hemodialysis
Address for correspondence: Dr. Uma Maheshwari K. No. 16/7A, Pavithra Flats, Thirupurkumaran Street, Radha Nagar, Chromepet, Chennai - 600 044, Tamil Nadu, India. E-mail: druma.neha@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The conventional, low flux (LF) dialyzer allows the removal of small molecular solutes like urea and creatinine. High flux (HF) dialyzers allow the effective removal of middle molecules (MM) as well, and are associated with reduced hemodialysis-related morbidity and mortality. Cystatin C has attractive characteristics as a representative MM. The aim of this study was to determine cystatin C reduction ratio (CysCRR) in both LF and HF groups and to compare it with other markers of dialysis adequacy. Thirty-seven patients were subjected to both LF and HF hemodialysis 2 weeks apart. Serum urea, creatinine and cystatin C were measured pre- and post-dialysis. Cystatin C was measured by latex-enhanced immunoturbidimetry. Urea and creatinine reduction ratios were 72.3 ± 14.7% and 62.5 ± 13%, respectively in the LF group. The CysCRR was −9.7 ± 6.7% and 29.2 ± 11% in LF and HF hemodialysis, respectively. The statistically significant decrease in CysCRR in the HF group shows the effective clearance of MM by HF dialyzers. Hence, CysCRR could be applied to measure the MM clearance in HF hemodialysis. This study highlights the significance of cystatin C as an important dialysis adequacy marker replacing the conventional markers such as urea and creatinine in HF hemodialysis. Among the middle molecules cystatin C scores over beta-2 microglobulin.
Keywords
Cystatin C
high flux dialysis
middle molecules

Introduction
The uremic syndrome is attributable to the progressive retention of a large number of compounds called uremic retention solutes or uremic toxins. They include not only small plasma solutes, but also protein-bound solutes and middle molecules (MM)[1](molecular weight between 500 and 60,000 Da).
The conventional low flux (LF) dialyzer permits effective small solute clearance, but its clearance of MM is relatively lower. High flux (HF) dialyzer allows more efficient removal of small water-soluble uremic compounds as well as MM and ensures improved dialysis quality and reduces the short- and long-term hemodialysis-related complications. Dialysis with HF membranes result in a reduction in erythropoietin resistance, delay in loss of residual renal function, improved lipid profiles, specifically increased high-density lipoproteins cholesterol, lowered triglyceride levels and removal of advanced glycosylation end products, which have been implicated in the pathogenesis of atherosclerosis and dialysis-related amyloidosis.[2]
Serum creatinine is the most commonly used marker for assessing kidney function in patients with chronic kidney disease (CKD). The use of serum urea is recommended by the Kidney Disease Outcome Quality Improvement clinical practice guideline to assess dialysis clearance.[3] The urea and creatinine reduction ratios (CRR) that are commonly used can assess the removal of only small solutes by conventional hemodialysis.
Cystatin C is a single nonglycosylated polypeptide chain consisting of 120 amino acid residues with a molecular mass of 13 kD, which is in the MM range.[4] It is produced by all nucleated cells,[5] freely filtered at the glomerulus and virtually fully reabsorbed and metabolized by proximal tubular cells.[6789] Several studies have suggested that cystatin C is useful as a marker of hemodialysis toxin removal, since it has the attractive features as a representative MM.[1011]
Though HF dialyzers with improved MM clearance are widely used, urea and CRR are used to assess the dialysis adequacy. This study aims to assess whether cystatin C reduction ratio (CysCRR) can be used as an alternative indicator of MM clearance in HF hemodialysis.
Subjects and Methods
The study was approved by the human ethics committee of Sri Ramachandra Medical College and Research Institute (SRMC), Chennai, India, and written consent was obtained from all the participants. A total set of 37 patients of both sexes >18 years old was selected. All the patients were initially subjected to LF hemodialysis and then to HF hemodialysis 2 weeks later. The dialyzers used were F6HPS for LF and F60S for HF (Fresenius Medical Care).
All patients undergoing maintenance hemodialysis at SRMC, 3 times/week were included. The residual renal function of the patients was not known. Patients with thyroid dysfunction, malignancies, steroid therapy and HIV infection and pregnant women were excluded from the study. All the blood samples were collected before and after the second HD session of the week, according to the guidelines for HD adequacy.[12] Blood samples were collected and serum was stored at −70°C until assayed. Urea nitrogen was measured using urease–glutamate dehydrogenase method on the BioLis premium 24i analyzer manufactured by Tokyo Boeki Medical System, Japan. Serum creatinine was measured by the modified Jaffe's assay and serum cystatin C was measured by latex-enhanced immunoturbidimetry on the same analyzer.
The efficacy of dialysis was then assessed by calculating the reduction ratio for serum creatinine as shown below: CRR = 100 × (1-Ci/Co) where Ci and Co represent post-dialysis and pre-dialysis serum creatinine levels. The same formula is used for the calculation of urea and CysCRR.
SPSS 10 statistical software developed by IBM Corporation, United States was used for the analysis of the results. Student's t-test was used for the analysis of the pre- and post-dialysis samples of urea, creatinine and cystatin C. Student's t-test was also used to compare urea, creatinine and CysCRR between LF and HF hemodialysis groups.
Results
There is a statistically significant increase in the mean values of cystatin C from the pre-dialysis to the post-dialysis in the LF group [Table 1]. There is a statistically significant decrease in the mean values of cystatin C from the pre-dialysis to the post-dialysis [Table 2] in the HF group.
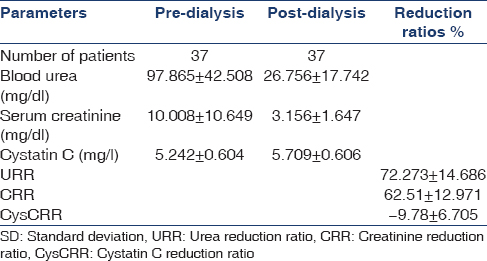
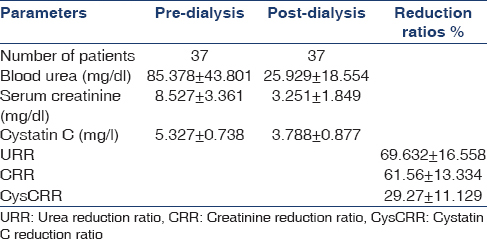
As shown in Figure 1, the difference in the mean values of CysCRR between the LF (−9.78 ± 6.705) and the HF (29.27 ± 11.129) dialysis is statistically significant.
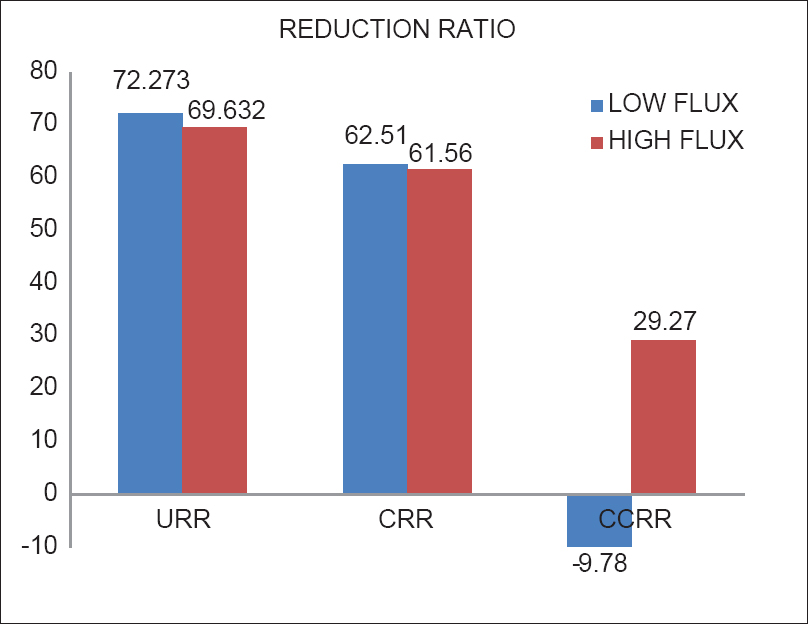
- Comparison of urea, creatinine and cystatin C reduction ratios between low flux and high flux hemodialysis
Discussion
Krishnamurthy et al., has shown statistically significant increase in the mean values of cystatin C with a CysCRR of −38% in the LF group. This increase in cystatin C values in the post-dialysis (LF) sample is due to the pore size of the LF membrane (1.5 nm), which does not allow the removal of MM like cystatin C. The electrostatic interaction between the microproteins and other plasma proteins adsorbed onto the dialyzer membrane hinders the filtration of these molecules. The rise in cystatin C is due to the hemoconcentration that occurs during dialysis.[13] Cystatin C serves as a surrogate marker of the inadequate clearance of MM by LF membranes.
The effective clearance of cystatin C by HF dialyzers is due to the difference in the ultrafiltration rates. Cystatin C is removed effectively by the HF membranes as the pore size of the membranes is between 1.5 and 1.7 nm.[14] Huang et al., found no correlation between CysCRR and the small solute clearance (urea reduction ratio and CRR). This is due to the difference in their intra-dialytic kinetic behavior.[15] Cystatin C, a MM that is distributed mainly extracellularly is minimally protein bound with presumed slow redistribution between the intravascular and the extravascular spaces because of its size. By contrast, serum urea and creatinine are distributed in extracellular (both intravascular and extravascular) and intracellular spaces, with presumed rapid equilibration between all three compartments during hemodialysis. CysCRR is affected by a combination of diffusive and convective clearance.
As cystatin C is strictly distributed in extracellular fluid, various kinetic models are not required to describe its kinetics during HD. Its production rate is relatively constant or minimally variable; cystatin C circulates freely in unbounded form and its elimination from the circulation is almost entirely through glomerular filtration.
Cystatin C has been shown to correlate with mortality in patients with coronary heart disease. In patients with stage III or IV CKD, the cystatin C level was associated with all cause and cardiovascular disease mortality.[16] It was concluded that if cystatin C levels correlate with clinical outcome in the dialysis population regardless of the residual renal function, it may become an important dialysis adequacy parameter.
Conclusion
This study highlights the importance of cystatin C as the dialysis adequacy marker for the clearance of MM in HF dialysis, thus replacing the conventional dialysis adequacy markers of urea and creatinine used in LF dialyzers.
Further studies with larger sample sizes are required to establish the target of a satisfactory cystatin C level after dialysis that is needed to improve the clinical outcomes in HF dialysis.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Review on uremic toxins: Classification, concentration, and interindividual variability. Kidney Int. 2003;63:1934-43.
- [Google Scholar]
- High flux and high efficiency procedures. In: Henrich WL, ed. Principles and Practice of Dialysis (4th ed). Philadelphia: Wolter and Kluwers Publishers; 2009. p. :126-8.
- [Google Scholar]
- Clinical practice guidelines and recommendations. Hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis. 2006;48:S1-322.
- [Google Scholar]
- Serum cystatin C measured by automated immunoassay: A more sensitive marker of changes in GFR than serum creatinine. Kidney Int. 1995;47:312-8.
- [Google Scholar]
- Monitoring renal function and limitations of renal function tests. Semin Nucl Med. 2008;38:32-46.
- [Google Scholar]
- Biochemistry and clinical role of human cystatin C. Crit Rev Clin Lab Sci. 2004;41:467-550.
- [Google Scholar]
- Glomerular filtration rate estimated by cystatin C among different clinical presentations. Kidney Int. 2006;69:399-405.
- [Google Scholar]
- Update on cystatin C: New insights into the importance of mild kidney dysfunction. Curr Opin Nephrol Hypertens. 2006;15:270-5.
- [Google Scholar]
- Factors influencing serum cystatin C levels other than renal function and the impact on renal function measurement. Kidney Int. 2004;65:1416-21.
- [Google Scholar]
- Could plasma cystatin C be useful as a marker of hemodialysis low molecular weight proteins removal? Nephron Clin Pract. 2004;98:c79-82.
- [Google Scholar]
- Cystatin C: A new marker of biocompatibility or a good marker for the redistribution of LMW proteins during hemodialysis? ASAIO Trans. 1988;34:202-4.
- [Google Scholar]
- Clinical practice guidelines for hemodialysis adequacy, update 2006. Am J Kidney Dis. 2006;48:S2-90.
- [Google Scholar]
- Effect of hemodialysis on circulating cystatin C levels in patients with end stage renal disease. Indian J Clin Biochem. 2010;25:43-6.
- [Google Scholar]
- Determinants of the serum concentrations of low molecular weight proteins in patients on maintenance hemodialysis. Kidney Int. 1994;45:1689-96.
- [Google Scholar]
- Cystatin C reduction ratio depends on normalized blood liters processed and fluid removal during hemodialysis. Clin J Am Soc Nephrol. 2011;6:319-25.
- [Google Scholar]
- Cystatin C and prognosis for cardiovascular and kidney outcomes in elderly persons without chronic kidney disease. Ann Intern Med. 2006;15(145):237-46.
- [Google Scholar]




