

Translate this page into:
Dimethyl Oxalate Exposure Induced Oxalate Nephropathy: A Trigger for Acute Kidney Injury
Corresponding author: Xiaoshuang Zhou, Department of Nephrology, Shanxi Provincial People Hospital, Taiyuan, China. E-mail: xiaoshuangzhou69@163.com
-
Received: ,
Accepted: ,
How to cite this article: Huang X, Liu F, Yuan H, Zhou X. Dimethyl Oxalate Exposure Induced Oxalate Nephropathy: A Trigger for Acute Kidney Injury. Indian J Nephrol. doi: 10.25259/IJN_816_2024
Dear Editor,
Dimethyl oxalate widely used as a raw material in developing countries for the organic synthesis of compounds such as ethanol, methyl glycolate, and ethylene glycol.1 We present a case of a previously healthy individual who developed acute kidney injury (AKI) following exposure to dimethyl oxalate.
A 33-year-old man presented to our hospital with abdominal pain, nausea, and vomiting for 30 hours. In recent years, he had provided technical support, like pipeline repair, at petrochemical factories. He had no history of dehydration, autoimmune disease, or surgical procedures. He denied habitual smoking or alcohol consumption. His vitals were stable: pulse rate was 78 beats/min, respiratory rate was 20/min, and blood pressure of 141/104 mmHg. He did not have fever. Laboratory investigations showed serum urea nitrogen level of 0.16 mg/dL (reference range, 0.026-0.079) and creatinine level of 714 (reference range, 53-106) µmol/L. Kidney biopsy [Figure 1] revealed multifocal tubular atrophy, eroded brush borders, and deposits of oxalate crystals within the tubules on polarized microscopy. He underwent hemodialysis and was prescribed 30 mg of prednisone daily. His renal function improved over the next few weeks.
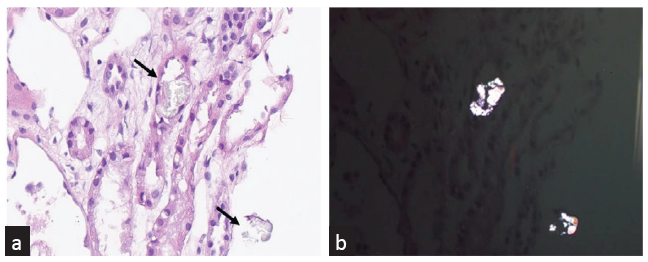
- (a) Oxalate nephropathy. The second patient kidney biopsy specimen show calcium oxalate crystals in tubules (black arrowheads). The crystals are clear on light microscopy (H&E stain; ×200). (b) Oxalate nephropathy. The same calcium oxalate crystals present bright birefringence when viewed by the polarizing light microscope (H&E stain; ×200). H&E: Hematoxylin and eosin.
When exposed to higher temperatures, dimethyl oxalate readily decomposes into oxalic acid. Once in the body, this acid binds with calcium, forming calcium oxalate crystals, which deposit within the kidney, causing AKI.2 The probable underlying mechanisms encompass oxalate-driven cytotoxicity within renal tubules and inflammation-mediated cell necrosis.3
Early detection and appropriate management could lead to a positive outcome and prevent its progression to more advanced renal disease.
Conflicts of interest
There are no conflicts of interest.
References
- Highly selective hydrogenation of dimethyl oxalate to methyl glycolate and ethylene glycol over an amino-assisted Ru-based catalyst. Chem Commun (Camb). 2022;58:11657-60.
- [CrossRef] [PubMed] [Google Scholar]
- Calcium oxalate crystal deposition in the kidney: Identification, causes and consequences. Urolithiasis. 2020;48:377-84.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Etiologies, clinical features, and outcome of oxalate nephropathy. Kidney Int Rep. 2020;5:1503-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




