

Translate this page into:
Finger nail creatinine and its role in confirming chronicity of renal failure
Address for correspondence: Dr. R. Kasi Visweswaran, Ananthapuri Hospitals and Research Institute, Trivandrum - 695 024, Kerala, India. E.mail: rkasivis@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
It is often difficult to differentiate acute renal failure (ARF) from chronic renal failure (CRF) when the patient presents with advanced uremia for the first time. Assessments of kidney size, history of nocturia, and pallor are used as indirect indicators of CRF. Some investigators have proposed an estimation of finger nail creatinine concentrations to differentiate between ARF and CRF, as patients with CRF have higher nail creatinine concentrations. Measurement of creatinine in the nail can be performed easily in a biochemistry laboratory. The nail clippings are cleaned, dried, pulverized and creatinine extracted from the powdered nail to be assessed biochemically. By standardizing the methods, the biochemistry laboratory can provide the results within 48 hours. In this study, we analyzed the nail clippings of 49 normal subjects, 50 cases of known acute kidney injury (AKI), and 50 cases of known CRF on follow-up at the Nephrology Clinic, Medical College, Trivandrum between December 1999 to November 2000. Forty-nine normal individuals were selected from healthy bystanders of respective patients. On study, it was revealed that patients with ARF had a mean fingernail creatinine level of 30.9 mg/100 g of nail as against 30.1 mg/100 g of nail in normal controls. There was no difference between the controls and ARF patients.Patients with known CRF had a mean fingernail creatinine level of 69.2 mg/100 g. There was a significant increase in the level of nail creatinine in patients with known CRF versus ARF patients and normal controls. The measurement of nail creatinine is useful, easy and can be standardized and performed in a biochemistry laboratory. This simple investigation can help in solving the question of ARF versus CRF in a given case. From this study, it is concluded that the result of creatinine concentrations of nail clippings can indicate chronicity of renal failure.
Keywords
Acute kidney injury
chronic renal failure
creatinine extraction
finger nail creatinine
toe nail creatinine

Introduction
The differentiation between acute renal failure (ARF) and chronic renal failure (CRF) in patients who present for the first time with uremia is often difficult, particularly because the past medical records are often not available. Levitt in 1965 for the first time suggested that the concentration of fingernail creatinine could be used as a marker of the duration of azotemia.[1] He found that patients with CRF had higher creatinine concentrations in the fingernails as compared to controls. Bergamo, et al., largely confirmed the findings of Levitt.[23] Sud, et al., also observed that the fingernail creatinine was significantly elevated in patients with known CRF and in those on maintenance hemodialysis compared to normal controls, ARF, and rapidly progressive glomerulonephritis (RPGN) patients as a group.[4] However, they observed large variability in the values of fingernail creatinine before concluding that the investigation is not a reliable indicator of the duration of uremia.[3] The method adopted to pulverize the nail was not mentioned and the variability could be related to drying and pulverization by mechanical means. As the studies suggest that the amount of creatinine that enters the fingernail plate during its formation is proportionate to the serum creatinine at the time of nail formation and remain unchanged till the full growth of the nail, proper standardization of the procedure could add to the benefits of the estimation.
In recent years, there has been a renewed interest in using fingernail creatinine concentration as a marker of the duration of azotemia.It has been known for over 60 years that measurable amounts of creatinine are present in fingernails and toenails.It has been postulated that concentration of creatinine in fingernail and toenail clippings might be of value in distinguishing acute from chronic uremia. If nail creatinine concentration is a reflection of the blood creatinine concentration at the time the nail was formed, then analysis of creatinine concentration of the clipped free edge of the nail which was formed many months earlier would provide a means of estimating the blood creatinine concentration which was present at that time. The optimum methodologies and techniques can be easily standardized. Creatinine enters the nail plate during the formation of the nail and its concentration is proportional to the serum creatinine at that time. Once incorporated into the nail, creatinine cannot be further added or removed till it grows and is clipped off. The creatinine is localized in the nail plate. The amounts of creatinine from the clippings at the tip of the nails represent the creatinine levels 4-6 months earlier. If the creatinine level in the nail clippings is higher than normal, it may suggest elevated serum creatininelevels 4-6 months earlier thus confirming chronicity. The present study was undertaken to examine and further explore the relationship between serum and fingernail creatinine and its application in determining the onset and duration of renal failure.
Any investigation that is not routinely done in a laboratory requires an initial effort to standardize the procedures and protocols. Assessment of fingernail creatinine in a biochemical laboratory is not very cumbersome and can easily be standardized.
The study was planned to answer the question whether AKI and CRF can be differentiated by assessing fingernail creatinine and standardizing a method for the assay.
Materials and Methods
A total of 149 subjects comprising three groups were included in the study. Forty-nine healthy volunteers from the bystanders of patients (32 males and 17 females) with a mean age of 43.46 years, 50 known patients with AKI (mean age 45.38 yrs) with no history of renal disease in the past, renal insufficiency of rapid onset, and recovery of renal function in a few weeks, and 50 known patients with chronic kidney injury (mean age 47.06 yrs) with irreversible and persistent azotemia of more than a duration of three months and whose levels of serum creatinine were above 6 mg/dL as per the previous medical records were chosen for the study. Groups 2 and 3 were patients admitted in the nephrology department.
To measure the growth velocity of fingernails in normal healthy volunteers, a mark was made on the surface of the fingernail at the posterior nail fold of the left index finger and the growth velocity was measured as the mark moved toward the free edge of the fingernail. For this, the growth velocity of nail in 12 staff members in the department were studied. For assessing fingernail versus toenail creatinine concentrations, fingernails and toenails from eight healthy volunteers were clipped simultaneously and stored separately in butter paper. The samples were then powdered, creatinine extracted, and assayed. For standardizing a method for pulverizing, the nail samples of 10 normal controls were processed by three different methods: (a) Powdering the nail using liquid nitrogen,(b) powdering the nail manually, and (c) dissolving the nail in potassium hydroxide (KOH).
In the present study, creatinine concentrations were measured on the fingernails of the same person with water bath temperature kept at 45°C and 37°C in 10 cases for selecting a proper temperature for the water bath. Likewise for selecting a suitable time interval for the water bath, fingernail creatinine concentrations of the same persons were measured by keeping the water bath temperature for 24 hours and 48 hours in 10 cases. For the purpose of standardizingthe method used for estimating the fingernail creatinine concentration, clippings from the free edge of the fingernails from all the fingers were obtained, labeled, and stored in butter paper until analysis. These cuttings were processed as one sample to obtain sufficient material for the extraction of measurable quantities of creatinine. In the laboratory, the nail clippings were washed free of dust particles, cleaned under running tap water, rinsed well in distilled water followed by acetone rinse, and dried. The clippings were placed in a small steel cylinder and frozen by adding liquid nitrogen to cover the clippings. The nitrogen was allowed to evaporate making the nail brittle. The nail was then powdered mechanically using a steel cylindrical rod. The procedure of freezing and powdering was repeated once or twice before all the nails were adequately powdered. The dry powdered nail was then weighed and placed in a 20 mL test tube containing 5 mL of distilled water and closedwith an airtight stopper. The creatinine was extracted by shaking the tube in a water bath, at 45°C for 24 hours. The aqueous extract was analyzed for creatinine using Jaffe's kinetic reaction method.
Other investigations like blood urea, serum creatinine, creatinine clearance, uric acid, total protein, albumin, phosphorous, sodium, and potassium were done in the blood samples of patients at the same time of collection of the nail samples.
Statistical analysis
Analysis of data from the estimation of fingernail creatinine was compared within the three groups by the Chi-square test H (X2).
Results
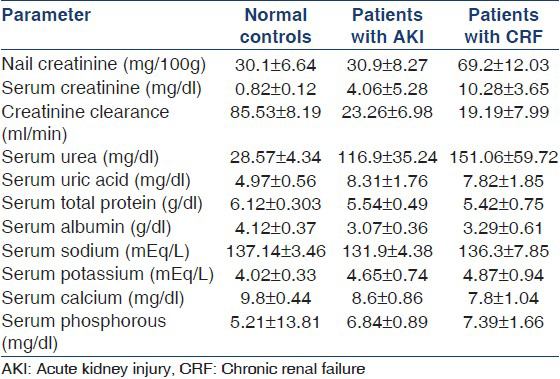
The nail creatinine and other biochemical parameters in the 49 normal controls, 50 cases of known AKI, and 50 cases of established CRF included in this study are given in Table 1.
Growth velocity of finger nails was studied in 12 normal healthy volunteers. The average number of days required for the growth from posterior nail fold to the tip was 116.83 ± 8.38 days. The difference between mean fingernail and toenail creatinine concentrations in eight healthy subjects studied was 30.53 mg and 30.50 mg/100 g of nail, respectively. The P value was >0.1, suggesting no statistically significant difference between the finger and toenail creatinine concentrations. Creatinine extraction was easily and optimally achieved using liquid nitrogen (technique I) compared to manual pulverization (technique II) and KOH extraction (technique III) [Figure 1].
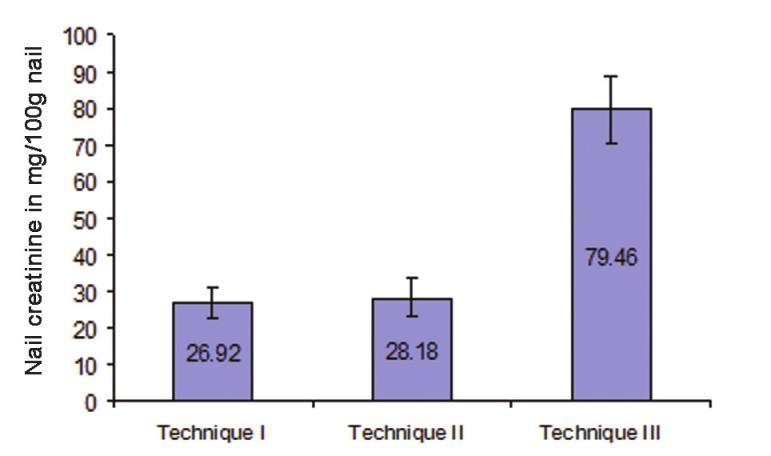
- Mean nail creatinine concentration between the three different methods of nail pulverization. The nail creatinine values were not significantly different between techniques I and II (P > 0.1), whereas they were statistically significant between techniques I and III as well as techniques II and III (P < 0.05). The high value obtained with technique III using potassium hydrochloride (KOH) is attributed to color chromogen interfering with Jaffe's test
Maintaining the temperature of the water bath at 45°C and agitation for 24 hours ensured maximum creatinine extraction from the pulverized nail [Figure 2].
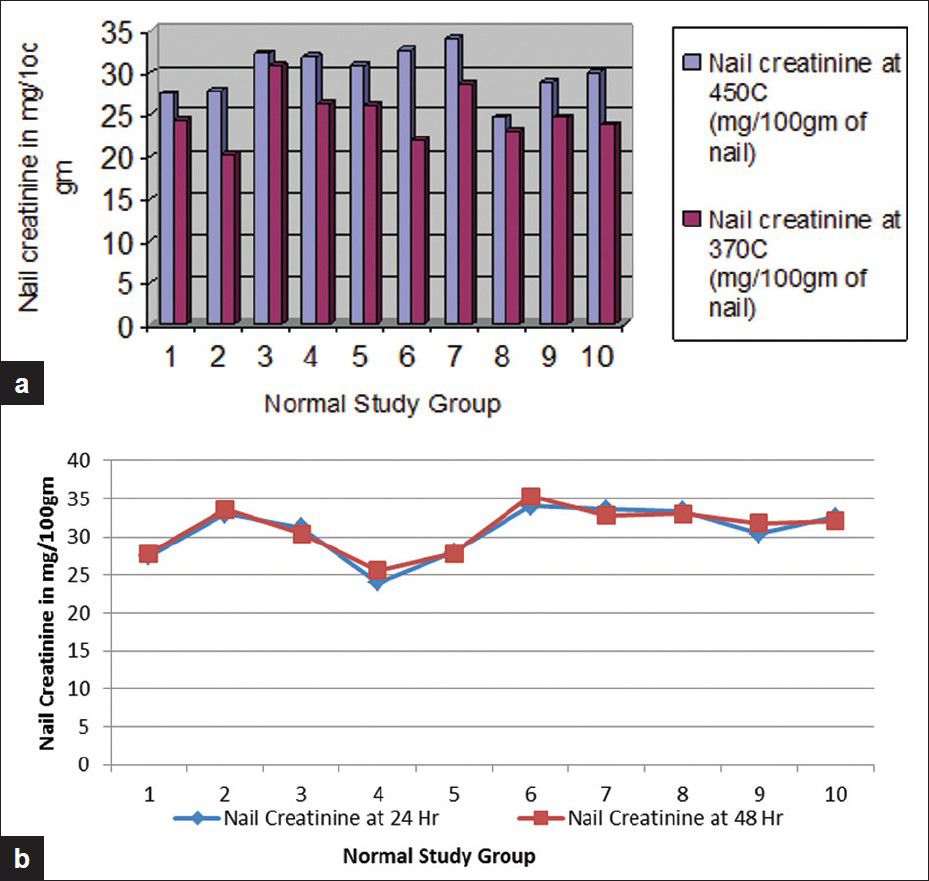
- Difference in creatinine levels at different temperatures (a) and different periods of agitation (b). The mean creatinine extraction at 45ºC was 30.01 mg/100 g and at 37ºC, 24.93 mg/100 g (P < 0.002), indicating ideal temperature of water bath as 45ºC. Mean nail concentration at 24 hours of agitation was 30.77 mg/100 g of nail, whereas at 48 hours it was 30.52 mg/100 g (P < 0.10), suggesting near-complete extraction from nail at 24 hours
The fingernail creatinine concentration was significantly higher in CRF patients compared to AKI patients and normal controls [Figure 3].
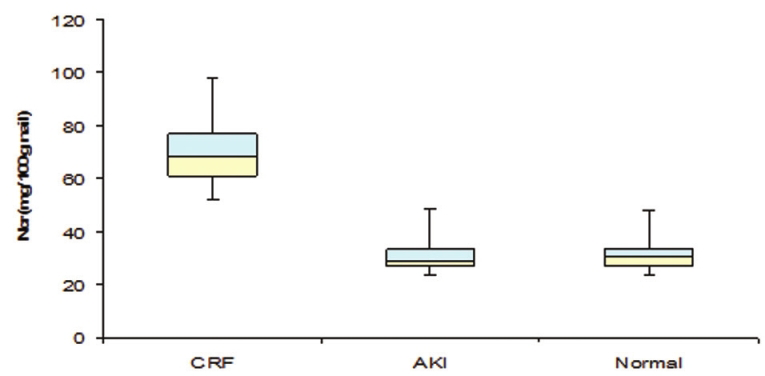
- Box plot showing nail creatinine levels in the three groups. The middle line within the box represents the median value. The upper and lower borders represent third and first quartile and the upper and lower ends of the whisker show the maximum and minimum values, respectively. The diagram clearly shows that patients with CRF have higher nail creatinine values compared to AKI and normal groups
Correlation of values of serum creatinine and nail clippings obtained at the same time are shown in Figure 4.
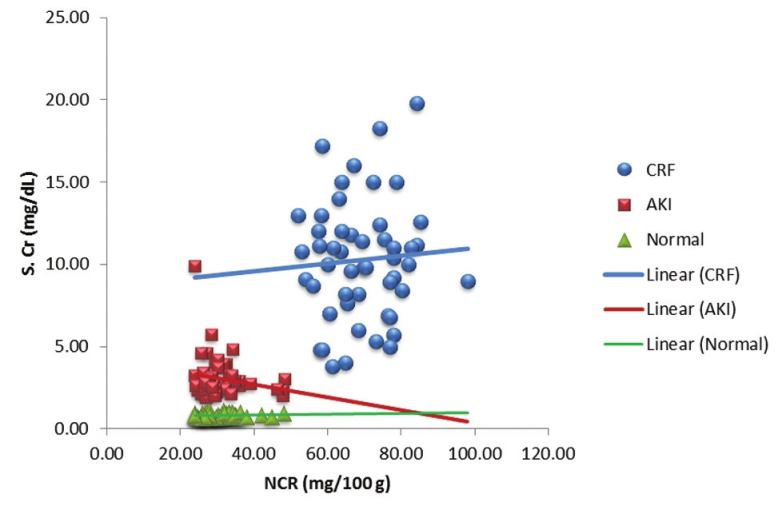
- Scatter diagram showing relationship between nail creatinine (NCr) and serum creatinine (SCr) levels. Nail creatinine levels in CRF are significantly high because the serum creatinine was higher at the time of formation of the nail 4-6 months earlier The solid line indicates the least squares regression line for the three groups. Blue line (CRF) indicates positive correlation, green line (normal controls) indicates positive correlation, and red line (AKI) indicates weak negative correlation
As the concentration of the nail creatinine from the free edges indicates the level of creatinine in the serum four to six months earlier, the presence of high nail creatinine combined with high serum creatinine suggests CRF.
Discussion
Measurement of creatinine in serum has been used to assess the severity of renal failure and for follow-up of renal functions. The creatinine level reflects the renal function at the time the specimen was obtained and does not indicate the duration of renal failure. Though physical examination, laboratory parameters, and assessment of kidney size by sonography are useful tools to differentiate between CRF and ARF, chronicity cannot be confirmed in all cases unless followed up for a few months. Estimation of fingernail creatinine can be performed in the biochemical laboratory after initial standardization and can be a useful tool to confirm chronicity of renal failure within 48 hours. If the concentration of nail creatinine is to be accepted as an indicator of the serum creatinine concentration at the time the nail was formed, then two conditions must be fulfilled.
Creatinine that is introduced into the nail root must remain unaltered in amount as the nail grows out. The amount of creatinine entering the forming nail must be proportional to the serum creatinine present at the time of formation.
Levitt[1] in his study explored the possibility that creatinine might leave an outgrowing nail by examining serial nail clippings of patients with chronic uremia after successful renal transplantation with reduction of serum creatinine to normal. If creatinine were lost from the nail plate either from the outside surface (for example, into water used during hand washing) or by diffusion from the inside surface to the vascular nail bed which is an area of low creatinine concentration, it would be expected that the nail creatinine concentration would fall concomitantly with a fall in blood levels. Instead, the nail creatinine remained elevated for at least a few months after the serum creatinine normalized. The possibility that creatinine might enter an outgrowing nail was investigated by examining nail clippings from patients who had normal renal function and who then became acutely uremic. The fact that nail creatinine concentration remained normal for weeks or months after the elevation of the serum creatinine concentration is evidence that creatinine does not passively diffuse from a nail bed with high creatinine concentration into a nail plate with low creatinine concentration.[1] This confirms that creatinine concentration in the nail reflects the blood creatinine at the time of nail formation and remains unchanged till the nail grows out and is clipped off. Therefore, the creatinine content of the clipped nail is a valid indicator of the serum creatinine that was present several months earlier and is of diagnostic importance in differentiating between ARF and CRF.
Bean[5] studied nail growth which showed that growth of the nail may be reduced by increasing age and chronic illness or increased by chronic trauma such as nail biting. On an average, approximately 100-130 days are required for a fingernail to be replaced after surgical or accidental avulsion. In the present study, the nail growth studied on 12 normal controls showed that the average number of days required for the nail to grow was 117 days (SD: 8.38). As the fingernail and toenail concentration are identical, both can be combined and utilized if adequate sampling is a problem. At least 20-30 mg of dry nail clippings are required for the assay.
The findings from the present study are similar to the result from Levitt, who described fingernail, and in a few instances toenail, creatinine concentration in normal individuals, and those with ARF and CRF. Pulverization using liquid nitrogen yields smooth powder and requires lesser effort compared to drying and manual powdering. Water bath temperature for nail creatinine extraction is taken as 45oC, as at this temperature, complete extraction of creatinine from the pulverized nail is achieved. Twenty-fourhours of agitation in the water bath helps to extract most of the creatinine and there is no additional benefit in extending the agitation time to 48 hours.
The study of fingernail creatinine concentration in these groups shows that the mean fingernail creatinine concentration in the normal control group was 30.1 ± 0.06 mg/100 g of nail. In ARF patients, it was 30.9 ± 1.17 mg/100 g of nail and in CRF, 69.2 ± 1.68 mg/100 g. There was no large variability as noted by Sud et al. In these groups, fingernail creatinine concentrations were estimated by a kinetic assay using Jaffe's principles for the estimationof creatinine and the intensity of color developed was estimated by kinetic assay on a semi-autoanalyzer.
From the study, the fingernail creatinine concentration in CRF is double vis-à-vis ARF. In the present study, there is a fairly distinct separation between fingernail creatinine concentration in ARF patients or normal individuals when compared with CRF patients. The results of the study indicate that fingernail creatinine concentration correlates well with serum creatinine levels present several months previously. In cases in which the duration of renal failure is unclear, the measurement of fingernail creatinine concentration may be a useful technique for differentiating between renal failure of recent onset or chronic duration. The test can be standardized in any biochemical laboratory and the results can be made available within 48 hours.
Just as glycated hemoglobin (HbA1c) helps us to assess the status of diabetic control that existed 2-3 months earlier, nail creatinine helps us get an idea about the elevation of creatinine that existed 4-6 months earlier. With some effort, this can be made a useful routine investigation.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Creatinine concentration of human fingernail and toenail clippings. Application in determining the duration of renal failure. Ann Intern Med. 1966;64:312-27.
- [Google Scholar]
- Fingernail creatinine as a predictor of prior renal function. Am J Kidney Dis. 1993;22:814-21.
- [Google Scholar]
- Can fingernail creatinine concentrations be used to predict duration of azotemia? Ren Fail. 1998;20:621-6.
- [Google Scholar]
- The measurement of fingernail creatinine in the differentiation of acute from chronic renal failure. Clin Nephrol. 1996;45:241-3.
- [Google Scholar]




