

Translate this page into:
Spontaneous callosal hemorrhage in a child on continuous ambulatory peritoneal dialysis
Address for correspondence: Prof. D. N. Gera, Department of Nephrology and Clinical Transplantation, Institute of Kidney Diseases and Research Centre, Dr. H L Trivedi Institute of Transplantation Sciences, Civil Hospital Campus, Ahmedabad - 380 016, Gujarat, India. E-mail: dineshgera@ymail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
An 8-year-old child on continuous ambulatory peritoneal dialysis was admitted with uncontrolled hypertension. His hemoglobin was 9 g/dl, platelets 2.5 lakhs/cmm, prothrombin time/activated partial thromboplastin time, and electrolytes were within normal limits. ELISA for hepatitis B surface antigen, HIV, and anti-hepatitis C virus were negative. After 2 days the child developed convulsion and cardiorespiratory arrest, after which he was resuscitated, intubated, shifted to the Intensive Care Unit, and put on invasive ventilatory support. His blood pressure was treated with noradrenaline infusion. On examination, the child was unconscious with Glasgow coma score of E1M2VT. His pupil was pinpoint and not reacting to light. Doll's eye movement was absent and was withdrawing to painful stimuli. Deep tendon reflexes were exaggerated with the presence of ankle clonus. Computed tomography brain was performed which showed patchy hemorrhages within the total length of the corpus callosum, more so in genu and splenium. There was no evidence of hydrocephalus or midline shift. Magnetic resonance imaging brain and magnetic resonance (MR) venogram of child was performed that showed areas of altered signal intensity in corpus callosum predominantly in genu and splenium, which appeared hyperintense on T1-weighted image and isointense on T2-fluid-attenuated inversion recovery images, which shows blooming on flicker fusion frequency images and diffusion restriction on diffusion weighted imaging, suggestive of early subacute hemorrhage [Figure 1]. On MR venogram, transverse sinus and other deep venous system were normal.
Patient could be weaned off from the ventilator after 4 days, but his Glasgow coma score did not improve.
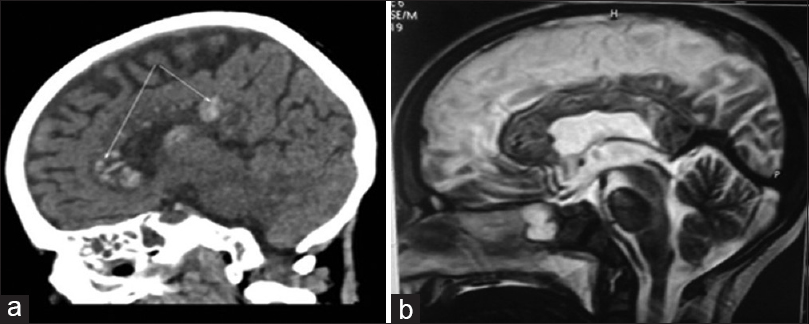
- (a) Computed tomography brain (noncontrast) shows patchy hemorrhages within whole length of corpus callosum, more so in genu and splenium (arrow). (b) Magnetic resonance imaging brain (T2-weighted sagittal view) shows areas of hypointense signal intensity in corpus callosum
Due to the dense compact nature of white matter tracts, it is vulnerable to shear injury in the event of trauma. Most of the callosal hemorrhages described in the literature are of elderly which are either associated with trauma or tumor or other etiological factors such as aneurysm of pericallosal artery or arteriovenous malformation.[12] There is a scarcity of data and rarity of occurrence of spontaneous callosal hemorrhage in Indian continent. Recently, two adult female patients had been described in association with deep cerebral venous sinus thrombosis from Bengaluru, India.[3] To the best of our knowledge and from PubMed search, it is the first reported case of callosal hemorrhage in pediatric age group in association with chronic kidney disease and hypertension.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Lesions of the corpus callosum: MR imaging and differential considerations in adults and children. AJR Am J Roentgenol. 2002;179:251-7.
- [Google Scholar]
- Arterial and venous vascularization of the corpus callosum. Neurochirurgie. 1998;44(1 Suppl):31-7.
- [Google Scholar]
- Corpus callosal hemorrhage due to deep cerebral venous sinus thrombosis. Neurol India. 2014;62:563-5.
- [Google Scholar]




