

Translate this page into:
Polycystic horseshoe kidney
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 34-year-old man was admitted with a history of fever, chill, rigor, and dysuria for 15 days. There was a history of abdominal pain in the right and left lumbar regions and in the hypogastric regions for 1 week. There was a history of vomiting for 4 days. Investigations revealed blood pressure of 120/80 mmHg, pulse rate 100 beats/min and oral temperature was 104°F. On examination, there was tenderness in all quadrants of the abdomen. Cardiovascular and respiratory system examination was unremarkable. Investigations revealed fasting blood glucose 107 mg/dL, serum creatinine 1.2 mg/dL, blood urea 78 mg/dL, serum sodium 134mEq/L, serum potassium 4.2 mEq/L, alanine transaminase 15 U/L, aspartate transaminase 21 U/L, serum alkaline phosphatase 263 U/L, bilirubin 0.6 mg/dL, serum proteins 7.5 g/dL, serum albumin 3.9 g/dL, haemoglobin 14.4 g/dL, total leukocyte count 15,200/cu. mm, differential cell count P70, L25, M4, E1%, platelet count 5.4 lakhs/ cu.mm, urine examination pH 5.00, specific gravity 1,030, albumin 2+, sugar nil, ketones negative, red blood cells nil, White blood cells 2-3/hpf, blood and urine cultures Escherichia coli. Ultrasound of the abdomen and computed tomography (CT) scan of the abdomen showed polycystic horse shoe kidney [Figure 1]. CT of the abdomen revealed cysts in the liver and spleen. The patient was treated according to the antibiogram. At 4 weeks, he was asymptomatic and serum creatinine was 1.4 mg/dL.
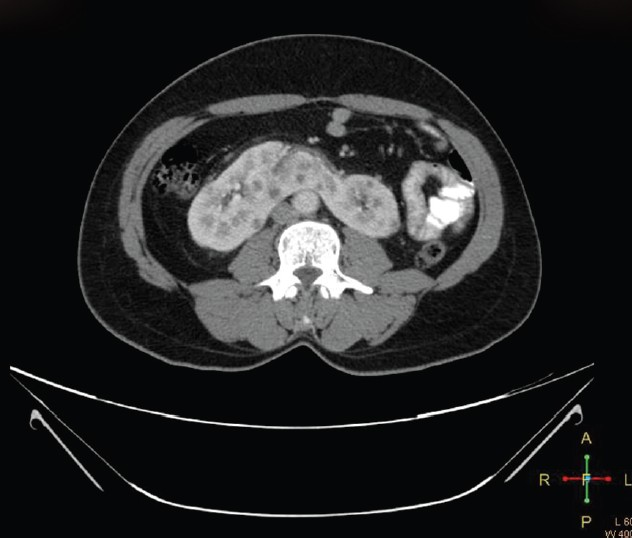
- Contrast-enhanced computed tomography scan of the abdomen shows multiple cysts in both kidneys suggestive of polycystic kidney disease. An isthmus joining the two kidneys anterior to the vertebrae is clearly visible. The isthmus also is riddled with cysts
About 20 patients of polycystic horseshoe kidney have been reported in the literature.[12] It is thought to represent two separate renal diseases. Horseshoe kidney is a renal fusion anomaly during embryogenesis; autosomal dominant polycystic kidney disease (ADPKD) is a hereditary disorder due to mutations in the genes responsible for the expression of the proteins polycystin 1 (ADPKD1) and polycystin 2 (ADPKD2). Horseshoe kidney occurs in 1 per 400-800 live births and ADPKD in 1 in 400-1,000 live births. Polycystic horseshoe kidney occurs 1 in 134 000 to 1 in 8 000 000 live births.[2] To date, no genetic association has been described between the ADPKD loci (PKD1 on chromosome 16 and PKD2 on chromosome 4) and horseshoe kidneys.
Source of Support: Nil
Conflict of Interest: None declared.




