

Translate this page into:
Renal Hypouricemia with Exercise Induced Acute Kidney Injury-A Case Report
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Acute kidney injury after exercise is most commonly secondary to rhabdomyolysis. Non-rhabdomyolysis AKI is secondary to a limited number of disorders of which renal hypouricemia (RHUC) needs a special mention. It is relatively a rare genetic disorder and is reported in Japanese and Ashkenazi Jews. Humans have lost the ability to metabolize uric acid as the “uricase” gene is suppressed. Renal tubules handle uric acid and aid in maintaining serum concentrations in the soluble range. Uric acid excretion is increased in RHUC patients due to proximal tubular defects. This leads to the loss of antioxidant capabilities of the kidney, predisposing them to severe AKI following anaerobic exercise. We report a case of exercise-induced AKI secondary to renal hypouricemia.
Keywords
AKI
exercise
loin pain
renal hypouricemia

Introduction
Acute kidney injury following severe exertion is a well described entity. Exercise-induced acute kidney injury (AKI) can be broadly categorized as[1] rhabdomyolysis associated and non-rhabdomyolysis AKI. Severe exertion can precipitate AKI secondary to rhabdomyolysis. Certain factors like trauma, alcohol, illicit drug use, infections, toxins, heat stroke, drugs like statins, and inflammatory myopathies enhance the risk.[2] The increased intracellular calcium leads to activation of proteases, mitochondrial dysfunction, and oxidative stress resulting in skeletal muscle cell death.[3] Excess myoglobin further causes nephrotoxicity.[4] Non-rhabdomyolysis AKI can be due to prerenal AKI, ATN secondary to dehydration, and NSAID use after strenuous exertion.
Renal hypouricemia with exercise-induced AKI is a rare entity described in the literature mainly from Japan and few cases from Europe. We describe a classic case of RHUC. Exercise-induced AKI associated with hypouricemia has an incidence of 0.12%–0.72% in Japanese literature[5] and very rare in other geographic areas. The diagnosis is based on biochemical markers like hypouricemia, increased fractional excretion of uric acid (FE-UA), and genetic testing. Here, we describe the case of a young adult with exercise-induced AKI caused by RHUC type 2. Urate concentration in the serum and urine may provide the initial indication of the defect in urate transporters before a molecular genetic analysis is performed
Case Report
A 15-year-old boy was referred to our hospital for raised creatinine. The illness started as extreme fatigue and severe bilateral loin pain following a sporting event at his school, where he participated in sprint run with other activities. His pain and fatigue worsened the next day and evaluation showed renal dysfunction. On admission, he was hemodynamically stable with a blood pressure of 130/90 mm of Hg and pulse rate of 90/minute. He had no signs of dehydration or muscle tenderness. He gave a history of oliguria for the past 12 hours but denied cola-colored urine, medication history, and drug abuse. He gave a history of similar illness 2 years ago, when his creatinine was 2.4 mg% and improved spontaneously over 2 weeks.
His preliminary evaluation showed severe azotemia (Urea 84 mg% and creatinine 7.4 mg%) with metabolic acidosis (serum bicarbonate 14.2 mEq/dL) and he progressively became anuric over the next 24 hours, despite fluid resuscitation and hemodialysis. Renal ultrasound/Doppler and non-contrast CT abdomen were unremarkable, only demonstrating slightly enlarged kidneys without any nephrolithiasis or hydronephrosis.
His routine urine analysis was unremarkable and serum electrolytes were normal; urine myoglobin was negative and serum CPK was 280 IU/ml. He required dialytic support for 10 days after which he slowly recovered. Prior AKI in a similar scenario, hypouricemia in the presence of renal dysfunction, family history of hypouricemia and the lierature review compelled us to consider hypouricemic AKI. We deferred the biopsy and creatinine normalized over the next 3 weeks.
His uric acid was noted to be extremely low and after looking into literature specific workup was directed at RHUC after renal recovery. Fractional excretion of uric acid was 52% (normal <10). Generalized proximal tubular dysfunction was not evident with no glycosuria or phosphaturia. Proximal tubular defects including Wilsons (Serum ceruloplasmin 27.14 mg/dL) and monoclonal gammopathy were excluded.
Genetic workup showed a compound heterozygous mutation at SLC2A9. A heterozygous 3% splice site variation in intron 9 of the SLC2A9 gene with an additional heterozygous missense variation in exon 5 of the SLC2A9 gene. This suggests a basolateral GLUT9 transporter anomaly which inhibits the transcellular transport of uric acid. Probenecid and pyrazinamide loading tests were not done in our patient as they are likely to yield positive result in URAT1 abnormality only. Meanwhile, his mother was tested for hypouricemia and found to have uric acid levels of 1.8 mg/dL.
Discussion
Uric acid, the product of purine metabolism is not further metabolized in humans and is excreted by kidneys and the gut. The evolutionary loss of uricase and the development of highly efficient resorptive mechanisms result in relative hyperuricemia in humans. Kidneys excrete two-thirds of the load and play a major role in urate homeostasis. After filtration, there is net reabsorption of up to 90% by the tubules mediated by a complex set of transport mechanisms. Recent understanding regarding the renal handling of uric acid in humans and some primates showed interesting observations. There are completely separate transport pathways for urate absorption and secretion across epithelia as depicted in Figure 1.[6] The loss of function in either pathway results in hypouricemia or hyperuricemia, resulting in varied phenotypic manifestations.
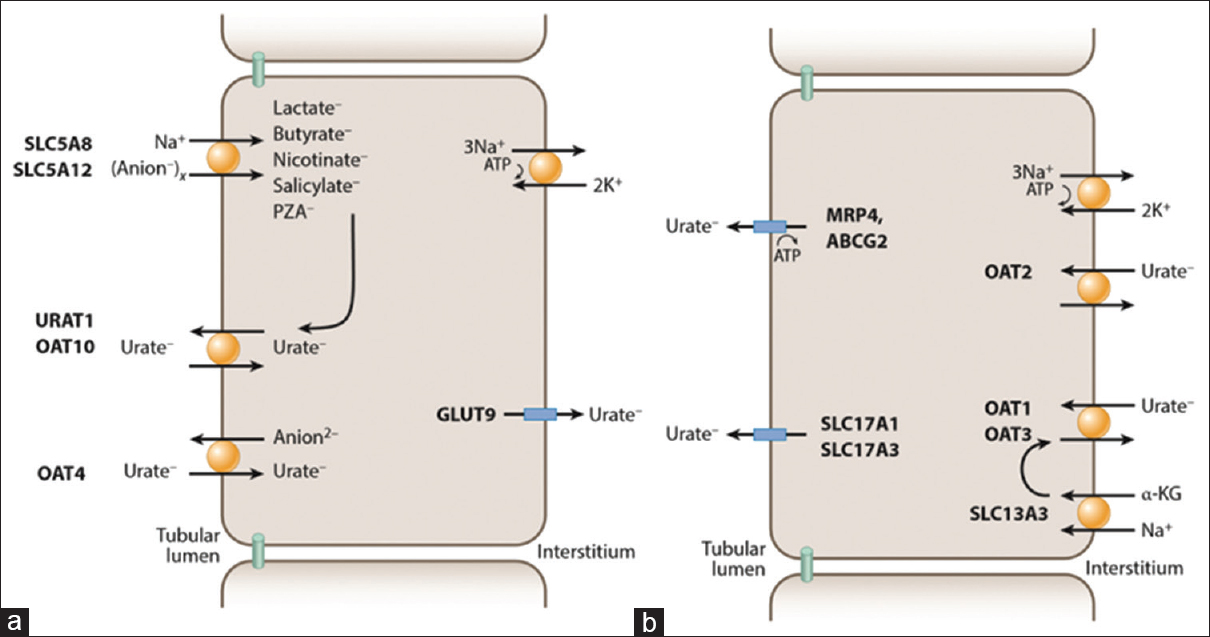
- Transport pathways for urate in proximal tubule cells. (a) Urate reabsorption. Na+-dependent anion transport by SLC5A8 and SLC5A12 increases intracellular concentrations of anions. They exchange with luminal urate via URAT1/OAT10. OAT4 appears to exchange urate with divalent anions. GLUT9 is the exit pathway for urate at the basolateral membrane. PZA denotes pyrazinoate. (b) Urate secretion. Urate enters the cell at the basolateral membrane via exchange with α-ketoglutarate (α-KG), through OAT1 and OAT3, or via OAT2; At the apical membrane, urate is secreted via MRP4, ABCG2, NPT1, and/or NPT . Courtesy of David B Mount[6]
Hypouricemia is defined as serum uric acid level below 2 mg/dL.[7] Idiopathic renal hypouricemia with AKI as genetic disorder was first reported by Erley et al.[8] in 1989 and subsequently many cases have been reported in Japanese and non-Ashkenazi Jews. Most of the patients are asymptomatic and are predisposed to exercise-induced AKI. Although the initial reports attributed renal injury to urate nephropathy and interstitial nephritis, subsequent reports from Japan[7910] described acute tubular necrosis (ATN) as the predominant mechanism of renal injury. The mechanisms by which RHUC predisposes to ATN are not clearly known.
Uric acid is a powerful antioxidant and free radical scavenger.[11] The low uric acid reabsorption in RHUC results in lower intracellular uric acid pool particularly in the proximal tubular epithelium.[12]
The three predominant mechanisms for AKI are
-
Decreased renal perfusion during exercise[9]
-
Ischemia reperfusion injury of the renal tubules resulting in free radical production[13]
-
Inability of the kidney to tackle the oxidative stress due to low intracellular uric acid pool.
Patients with renal hypouricemia present with severe loin pain and normal or only slightly elevated concentrations of CPK after anaerobic exercise. Our patient had a typical presentation with the precipitating event being a sprint run at his school. Ishikawa et al. in their detailed review of “Exercise induced Acute renal failure” defined the criteria for a syndromic diagnosis of ALPE (acute renal failure with loin pain after exertion).[5]
-
Recent intense anaerobic exercise
-
Normal or mildly elevated serum CPK and urine myoglobin
-
Severe loin pain several hours after exercise
Two types of transport anomalies can cause Renal hypouricemia. RHUC type 1 is caused by mutations in the gene SLC22A12, coding for human urate transporter 1(URAT1).[14] This was identified by Enomoto et al.[15] and constitutes a majority of the cases reported from Japan. RHUC type 2 is due to mutations in the gene SLC2A9, which encodes a high-capacity basolateral urate transporter (GLUT9).[1617] Our patient falls into the category of RHUC type 2, which is extremely rare as he was noted to have compound heterozygous mutation in the gene coding GLUT 9. Similar heterozygous mutations have been reported by Matsuo et al.[18] There is no definitive therapy. The prevention of anaerobic exercises like sprint racing and swimming can help. Few case reports suggested benefit with allopurinol.[19]
To the best of our knowledge, only a single case has been reported in Indian literature, where the patient had concomitant rhabdomyolysis and no genetic analysis was done.[20] Our case report is unique as it is the first Indian report where genetic workup was done which suggested a rare SLCA9 variant of RHUC.
Conclusion
RHUC is a very rare genetic abnormality resulting in ATN after anaerobic exercise. High index of suspicion is necessary for making this diagnosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Acute renal failure with severe loin pain and patchy renal ischemia after anaerobic exercise in patients with or without renal hypouricemia. Nephron. 2002;91:559-70.
- [Google Scholar]
- The syndrome of rhabdomyolysis: Pathophysiology and diagnosis. Eur J Intern Med. 2007;18:90-100.
- [Google Scholar]
- Acute kidney injury due to rhabdomyolysis and renal replacement therapy: A critical review. Crit Care Lond Engl. 2014;18:224.
- [Google Scholar]
- I. Exercise induced Acute Renal Failure- Acute Renal Failure with Severe Loin Pain and Patchy Renal Ischemia after Anaerobic Exercise. Tokyo, Japan: Springer; 2007. p. :1-108.
- The molecular physiology of uric acid homeostasis. Annu Rev Physiol. 2015;77:323-45.
- [Google Scholar]
- A case of exercise-induced acute renal failure with G774a mutation in Scl22a12 causing renal hypouricemia. J Korean Med Sci. 2011;26:1238-40.
- [Google Scholar]
- Acute renal failure due to uric acid nephropathy in a patient with renal hypouricemia. Klin Wochenschr. 1989;67:308-12.
- [Google Scholar]
- Exercise-induced acute renal failure in 3 patients with renal hypouricemia. Nihon Jinzo Gakkai Shi. 1990;32:923-8.
- [Google Scholar]
- [Two cases of exercise-induced acute renal failure with idiopathic renal hypouricemia] Nihon Jinzo Gakkai Shi. 2001;43:384-8.
- [Google Scholar]
- Uric acid provides an antioxidant defense in humans against oxidant- and radical-caused aging and cancer: A hypothesis. Proc Natl Acad Sci U S A. 1981;78:6858-62.
- [Google Scholar]
- Patients with renal hypouricemia are prone to develop acute renal failure--why? Clin Nephrol. 1995;43:207-8.
- [Google Scholar]
- Oxygen-derived free radicals in postischemic tissue injury. N Engl J Med. 1985;312:159-63.
- [Google Scholar]
- Molecular identification of a renal urate anion exchanger that regulates blood urate levels. Nature. 2002;417:447-52.
- [Google Scholar]
- SLC2A9 is a newly identified urate transporter influencing serum urate concentration, urate excretion and gout. Nat Genet. 2008;40:437-42.
- [Google Scholar]
- Homozygous SLC2A9 mutations cause severe renal hypouricemia. J Am Soc Nephrol JASN. 2010;21:64-72.
- [Google Scholar]
- Mutations in glucose transporter 9 gene SLC2A9 cause renal hypouricemia. Am J Hum Genet. 2008;83:744-51.
- [Google Scholar]
- Hereditary renal hypouricemia: A new role for allopurinol? Am J Med. 2014;127:e3-4.
- [Google Scholar]
- A young patient of hereditary renal hypouricaemia presenting with exercise-induced rhabdomyolysis and acute kidney injury. Ann Clin Biochem. 2013;50:271-3.
- [Google Scholar]




